

ご利用について
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about cancer genetics risk assessment and counseling. It is intended as a resource to inform and assist clinicians who care for cancer patients. It does not provide formal guidelines or recommendations for making health care decisions.
This summary is reviewed regularly and updated as necessary by the PDQ Cancer Genetics Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
CONTENTS
- Executive Summary
-
This executive summary reviews the topics covered in this PDQ summary on cancer genetics risk assessment and genetic counseling, with hyperlinks to detailed sections below that describe the evidence on each topic.
- Introduction
-
[Note: Many of the medical and scientific terms used in this summary are found in the NCI Dictionary of Genetics Terms. When a linked term is clicked, the definition will appear in a separate window.]
[Note: A concerted effort is being made within the genetics community to shift terminology used to describe genetic variation. The shift is to use the term “variant” rather than the term “mutation” to describe a difference that exists between the person or group being studied and the reference sequence, particularly for differences that exist in the germline. Variants can then be further classified as benign (harmless), likely benign, of uncertain significance, likely pathogenic, or pathogenic (disease causing). Throughout this summary, we will use the term pathogenic variant to describe a disease-causing mutation. Refer to the Cancer Genetics Overview summary for more information about variant classification.]
This summary describes current approaches to assessing and counseling people about their chance of having an inherited susceptibility to cancer. Genetic counseling is defined by the National Society of Genetic Counselors as the process of helping people understand and adapt to the medical, psychological, and familial implications of genetic contributions to disease. Several reviews present overviews of the cancer risk assessment, counseling, and genetic testing process.[ 1 ][ 2 ]
Individuals are considered to be candidates for cancer risk assessment if they have a personal and/or family history (maternal or paternal lineage) with features suggestive of hereditary cancer.[ 1 ] These features vary by type of cancer and specific hereditary syndrome. Criteria have been published to help identify individuals who may benefit from genetic counseling.[ 1 ][ 3 ] The PDQ cancer genetics information summaries on breast, ovarian, endometrial, colorectal, prostate, kidney, and skin cancers and endocrine and neuroendocrine neoplasias describe the clinical features of hereditary syndromes associated with these conditions.
The following are features that suggest hereditary cancer:[ 4 ][ 5 ][ 6 ][ 7 ][ 8 ]
As part of the process of genetic education and counseling, genetic testing may be considered when the following factors are present:[ 9 ][ 10 ][ 11 ]
It is important that individuals who are candidates for genetic testing undergo genetic education and counseling before testing to facilitate informed decision making and adaptation to the risk or condition.[ 1 ][ 7 ][ 8 ][ 9 ][ 10 ][ 11 ][ 12 ][ 13 ] Genetic education and counseling allows individuals to consider the various medical uncertainties, diagnosis, or medical management based on varied test results, and the risks, benefits, and limitations of genetic testing.
参考文献- Riley BD, Culver JO, Skrzynia C, et al.: Essential elements of genetic cancer risk assessment, counseling, and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns 21 (2): 151-61, 2012.[PUBMED Abstract]
- Weitzel JN, Blazer KR, MacDonald DJ, et al.: Genetics, genomics, and cancer risk assessment: State of the Art and Future Directions in the Era of Personalized Medicine. CA Cancer J Clin 61 (5): 327-59, 2011 Sep-Oct.[PUBMED Abstract]
- Hampel H, Bennett RL, Buchanan A, et al.: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 17 (1): 70-87, 2015.[PUBMED Abstract]
- Tobias DH, Eng C, McCurdy LD, et al.: Founder BRCA 1 and 2 mutations among a consecutive series of Ashkenazi Jewish ovarian cancer patients. Gynecol Oncol 78 (2): 148-51, 2000.[PUBMED Abstract]
- Beller U, Halle D, Catane R, et al.: High frequency of BRCA1 and BRCA2 germline mutations in Ashkenazi Jewish ovarian cancer patients, regardless of family history. Gynecol Oncol 67 (2): 123-6, 1997.[PUBMED Abstract]
- Gabai-Kapara E, Lahad A, Kaufman B, et al.: Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A 111 (39): 14205-10, 2014.[PUBMED Abstract]
- Randall LM, Pothuri B, Swisher EM, et al.: Multi-disciplinary summit on genetics services for women with gynecologic cancers: A Society of Gynecologic Oncology White Paper. Gynecol Oncol 146 (2): 217-224, 2017.[PUBMED Abstract]
- Committee on Practice Bulletins–Gynecology, Committee on Genetics, Society of Gynecologic Oncology: Practice Bulletin No 182: Hereditary Breast and Ovarian Cancer Syndrome. Obstet Gynecol 130 (3): e110-e126, 2017.[PUBMED Abstract]
- Robson ME, Storm CD, Weitzel J, et al.: American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol 28 (5): 893-901, 2010.[PUBMED Abstract]
- Lancaster JM, Powell CB, Chen LM, et al.: Society of Gynecologic Oncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol 136 (1): 3-7, 2015.[PUBMED Abstract]
- Robson ME, Bradbury AR, Arun B, et al.: American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. J Clin Oncol 33 (31): 3660-7, 2015.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 1.2020. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed December 23, 2019.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal. Version 3.2019. Plymouth Meeting, PA: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed February 05, 2020.[PUBMED Abstract]
- Identification of Candidates for Referral to Genetic Counseling
-
After an individual’s personal and family cancer histories have been collected, several factors could warrant referral to a genetics professional for evaluation of hereditary cancer susceptibility syndromes. The American College of Medical Genetics and Genomics and the National Society of Genetic Counselors have published a comprehensive set of personal and family history criteria to guide the identification of at-risk individuals and appropriate referral for cancer genetic risk consultation.[ 1 ] These practice guidelines take into account tumor types or other features and related criteria that would indicate a need for a genetics referral. The authors state that the guidelines are intended to maximize appropriate referral of at-risk individuals for cancer genetic consultation but are not meant to provide genetic testing or treatment recommendations.
Tools to Identify Candidates for Genetic Counseling and Genetic Testing
Identification of patients at moderate to high risk of hereditary cancer for genetic services is recommended by all major societies. Primary care physicians have a number of tools available to triage patients. In addition to the published categorical guidelines available through professional organizations,[ 1 ][ 2 ][ 3 ][ 4 ] there are also red flag cards, paper-based checklists, and patient-directed online referral tools. Table 1 provides a list of several publically available resources that can be used to identify patients for referral to genetic services. Although most tools are brief and simple enough for patients to complete on their own, either previsit, online, or in the waiting room, clinical review is warranted. Many include the commonly known features suggestive of hereditary cancers, but exclusions are noted in the table below.
Table 1. Available Tools to Identify Candidates for Referral to Genetics for Further Evaluation and Consideration of Genetic Testing Name Mode and Length (Referral Threshold) / Tool Completed By (Tested Setting) Features aAll tools are available in English. Tools were tested in U.S. populations unless otherwise stated. bReferral yield in test population. Breast/Ovarian Cancer Tools for Health Professionals Breast cancer referral screening tool (B-RST) [ 5 ] • Paper or Online Sensitivity 81%/Specificity 92% Health professional (mammography clinic) Does not include bilateral breast cancer or breast and ovarian cancer in the same person. 6% high riskb. • 2-column table (2 positive answers) Validated in other populations [ 6 ][ 7 ][ 8 ] Family health screening questionnaire [ 9 ] • Paper Sensitivity 95%/Specificity 54% Health professional (primary care) Tested in Australia. Does not include bilateral breast cancer or breast and ovarian cancer in the same person. • 9 questions (1 positive answer) Family history assessment tool (FHAT) [ 10 ] • Paper Not provided Health professional (primary care) Tested in Canada. Includes colon and prostate cancers. Includes third-degree relatives. • 12 questions (>10 points for family score) FHS-7 [ 11 ] • Paper Sensitivity 87%/Specificity 54% Health professional (primary care) Tested in community-based population in Brazil. 6% high riskb. • 7 questions (1 positive answer) Pedigree assessment tool (PAT) [ 12 ] • Paper Sensitivity 100%/Specificity 93% Health professional (primary care) Tested in community hospital. • 5 items (≥8 points) Validated in other populations [ 13 ] Breast/Ovarian Cancer Tools for Patients “Are you at risk for hereditary breast cancer?” educational brochure [ 14 ] • Paper Not provided Patient (breast and cervical cancer screening clinic) Tested in underinsured or uninsured low-income women. • 11 questions (1 positive answer) Family history questionnaire [ 15 ] • Paper Not provided Patient (mammography clinic) Tested in Australia. Does not include ovarian cancer, male breast cancer, or bilateral breast cancer. 13% high riskb. • 6 questions (about 3 positive answers) 6-point scale [ 16 ] • Paper Sensitivity 27%/Specificity 97% Patient (mammography clinic) Tested in low-income women in a safety net setting. • 10 questions (≥6 points) Colon Cancer Tools FHS-7 [ 11 ] • Paper Sensitivity 87%/Specificity 54% Health professional (primary care) Tested in community-based population in Brazil. 6% high riskb. • 7 questions (1 positive answer) Lynch syndrome risk assessment tool [ 17 ] • Paper Not provided Patient (colonoscopy clinic) 3% high riskb. • 7 questions (1 positive answer) There are also more extensive statistical risk assessment models designed for both highly motivated patients [ 18 ][ 19 ] and genetic specialists (e.g., CancerGene, IBIS).
参考文献- Hampel H, Bennett RL, Buchanan A, et al.: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 17 (1): 70-87, 2015.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 1.2020. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed December 23, 2019.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal. Version 3.2019. Plymouth Meeting, PA: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed February 05, 2020.[PUBMED Abstract]
- Lancaster JM, Powell CB, Chen LM, et al.: Society of Gynecologic Oncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol 136 (1): 3-7, 2015.[PUBMED Abstract]
- Bellcross CA, Lemke AA, Pape LS, et al.: Evaluation of a breast/ovarian cancer genetics referral screening tool in a mammography population. Genet Med 11 (11): 783-9, 2009.[PUBMED Abstract]
- Bellcross C: Further development and evaluation of a breast/ovarian cancer genetics referral screening tool. Genet Med 12 (4): 240, 2010.[PUBMED Abstract]
- Brannon Traxler L, Martin ML, Kerber AS, et al.: Implementing a screening tool for identifying patients at risk for hereditary breast and ovarian cancer: a statewide initiative. Ann Surg Oncol 21 (10): 3342-7, 2014.[PUBMED Abstract]
- Bellcross C, Hermstad A, Tallo C, et al.: Validation of Version 3.0 of the Breast Cancer Genetics Referral Screening Tool (B-RST™). Genet Med 21 (1): 181-184, 2019.[PUBMED Abstract]
- Emery JD, Reid G, Prevost AT, et al.: Development and validation of a family history screening questionnaire in Australian primary care. Ann Fam Med 12 (3): 241-9, 2014 May-Jun.[PUBMED Abstract]
- Gilpin CA, Carson N, Hunter AG: A preliminary validation of a family history assessment form to select women at risk for breast or ovarian cancer for referral to a genetics center. Clin Genet 58 (4): 299-308, 2000.[PUBMED Abstract]
- Ashton-Prolla P, Giacomazzi J, Schmidt AV, et al.: Development and validation of a simple questionnaire for the identification of hereditary breast cancer in primary care. BMC Cancer 9: 283, 2009.[PUBMED Abstract]
- Hoskins KF, Zwaagstra A, Ranz M: Validation of a tool for identifying women at high risk for hereditary breast cancer in population-based screening. Cancer 107 (8): 1769-76, 2006.[PUBMED Abstract]
- Teller P, Hoskins KF, Zwaagstra A, et al.: Validation of the pedigree assessment tool (PAT) in families with BRCA1 and BRCA2 mutations. Ann Surg Oncol 17 (1): 240-6, 2010.[PUBMED Abstract]
- Cohn WF, Jones SM, Miesfeldt S: "Are you at risk for hereditary breast cancer?": development of a personal risk assessment tool for hereditary breast and ovarian cancer. J Genet Couns 17 (1): 64-78, 2008.[PUBMED Abstract]
- Fisher TJ, Kirk J, Hopper JL, et al.: A simple tool for identifying unaffected women at a moderately increased or potentially high risk of breast cancer based on their family history. Breast 12 (2): 120-7, 2003.[PUBMED Abstract]
- Stewart SL, Kaplan CP, Lee R, et al.: Validation of an Efficient Screening Tool to Identify Low-Income Women at High Risk for Hereditary Breast Cancer. Public Health Genomics 19 (6): 342-351, 2016.[PUBMED Abstract]
- Rabinowitz-Abrams D, Morgan D, Morse J, et al.: Building a tool to identify risk for Lynch syndrome among individuals presenting for screening colonoscopy. J Genet Couns 19 (4): 353-9, 2010.[PUBMED Abstract]
- Sweet K, Sturm AC, Rettig A, et al.: Clinically relevant lessons from Family HealthLink: a cancer and coronary heart disease familial risk assessment tool. Genet Med 17 (6): 493-500, 2015.[PUBMED Abstract]
- Baumgart LA, Postula KJ, Knaus WA: Initial clinical validation of Health Heritage, a patient-facing tool for personal and family history collection and cancer risk assessment. Fam Cancer 15 (2): 331-9, 2016.[PUBMED Abstract]
- Cancer Risk Assessment and Counseling
-
Comprehensive cancer risk assessment is a consultative service that includes clinical assessment, genetic testing when appropriate, and risk management recommendations delivered in the context of one or more genetic counseling sessions. Pretest genetic counseling is an important part of the risk assessment process and helps patients understand their genetic testing options and potential outcomes. Posttest genetic counseling helps patients understand their test results, including the medical implications for themselves and their relatives.
The following professional organizations emphasize the importance of genetic counseling in the cancer risk assessment and genetic testing process:
A list of organizations that have published clinical practices guidelines related to genetic counseling, risk assessment, genetic testing, and/or management for hereditary breast and ovarian cancers is available in the PDQ summary on Genetics of Breast and Gynecologic Cancers.
Genetic counseling informs the consultand about potential cancer risks and the benefits and limitations of genetic testing and offers an opportunity to consider the potential medical, psychological, familial, and social implications of genetic information.[ 9 ][ 18 ] Descriptions of genetic counseling and the specialized practice of cancer risk assessment counseling are detailed below.
Genetic Counseling
Genetic counseling has been defined by the National Society of Genetic Counselors as the process of helping people understand and adapt to the medical, psychological, and familial implications of genetic contributions to disease, including the following:[ 9 ]
Traditionally, genetic counseling services have been delivered using individualized in-person appointments. However, other methodologies have been implemented, including group sessions, telephone counseling, and online genetic counseling using remote videoconferencing, which is often referred to as telegenetics. (Refer to the Modalities of genetic counseling section of this summary for more information.)
Central to the philosophy and practice of genetic counseling are the principles of voluntary utilization of services, informed decision making, attention to psychosocial and affective dimensions of coping with genetic risk, and protection of patient confidentiality and privacy. This is facilitated through a combination of rapport building and information gathering; establishing or verifying diagnoses; risk assessment and calculation of quantitative occurrence/recurrence risks; education and informed consent processes; psychosocial assessment, support, and counseling appropriate to a family’s culture and ethnicity; and other relevant background characteristics.[ 19 ][ 20 ] The psychosocial assessment is especially important in the genetic counseling process because individuals most vulnerable to adverse effects of genetic information may include those who have had difficulty dealing with stressful life events in the past.[ 21 ] Variables that may influence psychosocial adjustment to genetic information include individual and familial factors; cultural factors; and health system factors such as the type of test, disease status, and risk information.[ 21 ] Findings from a psychosocial assessment can be used to help guide the direction of the counseling session.[ 10 ] An important objective of genetic counseling is to provide an opportunity for shared decision making when the medical benefits of one course of action are not demonstrated to be superior to another. The relationship between the availability of effective medical treatment for carriers of pathogenic variants and the clinical validity of a given test affects the degree to which personal choice or physician recommendation is supported in counseling at-risk individuals.[ 22 ] Uptake of genetic counseling services among those referred varies based on the cancer syndrome and the clinical setting. Efforts to decrease barriers to service utilization are ongoing (e.g., the use of a patient navigator or an oncology clinic–based genetic counselor may increase utilization of these services).[ 23 ][ 24 ][ 25 ] Readers interested in the nature and history of genetic counseling are referred to a number of comprehensive reviews.[ 26 ][ 27 ][ 28 ][ 29 ][ 30 ][ 31 ]
Pretest Genetic Education and Counseling Outcomes
Cancer risk assessment counseling has emerged as a specialized practice that requires knowledge of genetics, oncology, and individual and family counseling skills that may be provided by health care providers with this interdisciplinary training.[ 32 ] Some centers providing cancer risk assessment services involve a multidisciplinary team, which may include a genetic counselor; a genetics advanced practice nurse; a medical geneticist or a physician, such as an oncologist, surgeon, or internist; and a mental health professional.
参考文献- Hampel H, Bennett RL, Buchanan A, et al.: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 17 (1): 70-87, 2015.[PUBMED Abstract]
- Committee on Practice Bulletins–Gynecology, Committee on Genetics, Society of Gynecologic Oncology: Practice Bulletin No 182: Hereditary Breast and Ovarian Cancer Syndrome. Obstet Gynecol 130 (3): e110-e126, 2017.[PUBMED Abstract]
- Robson ME, Storm CD, Weitzel J, et al.: American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol 28 (5): 893-901, 2010.[PUBMED Abstract]
- Robson ME, Bradbury AR, Arun B, et al.: American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. J Clin Oncol 33 (31): 3660-7, 2015.[PUBMED Abstract]
- Botkin JR, Belmont JW, Berg JS, et al.: Points to Consider: Ethical, Legal, and Psychosocial Implications of Genetic Testing in Children and Adolescents. Am J Hum Genet 97 (1): 6-21, 2015.[PUBMED Abstract]
- Statement of the American Society of Human Genetics on genetic testing for breast and ovarian cancer predisposition. Am J Hum Genet 55 (5): i-iv, 1994.[PUBMED Abstract]
- International Society of Nurses in Genetics: Provision of Quality Genetic Services and Care: Building a Multidisciplinary, Collaborative Approach among Genetic Nurses and Genetic Counselors. Pittsburgh, Pa: International Society of Nurses in Genetics, 2006. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- International Society of Nurses in Genetics: Genetic Counseling for Vulnerable Populations: The Role of Nursing. Pittsburgh, Pa: International Society of Nurses in Genetics, 2010. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Resta R, Biesecker BB, Bennett RL, et al.: A new definition of Genetic Counseling: National Society of Genetic Counselors' Task Force report. J Genet Couns 15 (2): 77-83, 2006.[PUBMED Abstract]
- Riley BD, Culver JO, Skrzynia C, et al.: Essential elements of genetic cancer risk assessment, counseling, and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns 21 (2): 151-61, 2012.[PUBMED Abstract]
- Berliner JL, Fay AM, Cummings SA, et al.: NSGC practice guideline: risk assessment and genetic counseling for hereditary breast and ovarian cancer. J Genet Couns 22 (2): 155-63, 2013.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 1.2020. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed December 23, 2019.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal. Version 3.2019. Plymouth Meeting, PA: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed February 05, 2020.[PUBMED Abstract]
- Oncology nursing: the application of cancer genetics and genomics throughout the oncology care continuum. Oncol Nurs Forum 40 (1): 10-1, 2013.[PUBMED Abstract]
- Lancaster JM, Powell CB, Chen LM, et al.: Society of Gynecologic Oncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol 136 (1): 3-7, 2015.[PUBMED Abstract]
- Randall LM, Pothuri B, Swisher EM, et al.: Multi-disciplinary summit on genetics services for women with gynecologic cancers: A Society of Gynecologic Oncology White Paper. Gynecol Oncol 146 (2): 217-224, 2017.[PUBMED Abstract]
- Moyer VA; U.S. Preventive Services Task Force: Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 160 (4): 271-81, 2014.[PUBMED Abstract]
- Resta RG: Defining and redefining the scope and goals of genetic counseling. Am J Med Genet C Semin Med Genet 142C (4): 269-75, 2006.[PUBMED Abstract]
- Baty BJ, Kinney AY, Ellis SM: Developing culturally sensitive cancer genetics communication aids for African Americans. Am J Med Genet 118A (2): 146-55, 2003.[PUBMED Abstract]
- Jenkins JF, Lea DH: Nursing Care in the Genomic Era: A Case-Based Approach. Sudbury, Mass: Jones and Bartlett Publishers, 2005.[PUBMED Abstract]
- Meiser B, Gaff C, Julian-Reynier C, et al.: International perspectives on genetic counseling and testing for breast cancer risk. Breast Dis 27: 109-25, 2006-2007.[PUBMED Abstract]
- Burke W, Pinsky LE, Press NA: Categorizing genetic tests to identify their ethical, legal, and social implications. Am J Med Genet 106 (3): 233-40, 2001 Fall.[PUBMED Abstract]
- Rahm AK, Sukhanova A, Ellis J, et al.: Increasing utilization of cancer genetic counseling services using a patient navigator model. J Genet Couns 16 (2): 171-7, 2007.[PUBMED Abstract]
- Kentwell M, Dow E, Antill Y, et al.: Mainstreaming cancer genetics: A model integrating germline BRCA testing into routine ovarian cancer clinics. Gynecol Oncol 145 (1): 130-136, 2017.[PUBMED Abstract]
- Kishan AU, Gomez CL, Dawson NA, et al.: Increasing Appropriate BRCA1/2 Mutation Testing: The Role of Family History Documentation and Genetic Counseling in a Multidisciplinary Clinic. Ann Surg Oncol 23 (Suppl 5): 634-641, 2016.[PUBMED Abstract]
- Walker AP: The practice of genetic counseling. In: Baker DL, Schuette JL, Uhlmann WR, eds.: A Guide to Genetic Counseling. New York, NY: Wiley-Liss, 1998, pp 1-26.[PUBMED Abstract]
- Bartels DM, LeRoy BS, Caplan AL, eds.: Prescribing Our Future: Ethical Challenges in Genetic Counseling. New York, NY: Aldine De Gruyter, 1993.[PUBMED Abstract]
- Kenen RH: Genetic counseling: the development of a new interdisciplinary occupational field. Soc Sci Med 18 (7): 541-9, 1984.[PUBMED Abstract]
- Kenen RH, Smith AC: Genetic counseling for the next 25 years: models for the future. J Genet Couns 4 (2): 115-24, 1995.[PUBMED Abstract]
- Biesecker BB: Goals of genetic counseling. Clin Genet 60 (5): 323-30, 2001.[PUBMED Abstract]
- Weil Jon: Psychosocial Genetic Counseling. New York, NY: Oxford University Press, 2000.[PUBMED Abstract]
- Freedman AN, Wideroff L, Olson L, et al.: US physicians' attitudes toward genetic testing for cancer susceptibility. Am J Med Genet A 120A (1): 63-71, 2003.[PUBMED Abstract]
- Components of the Risk Assessment Process
-
This section provides an overview of critical elements in the cancer risk assessment process.
A number of professional guidelines on the elements of cancer genetics risk assessment and counseling are available.[ 1 ][ 2 ][ 3 ][ 4 ][ 5 ] Except where noted, the discussion below is based on these guidelines.
The cancer risk assessment and genetic counseling process consists of one or more consultative sessions and generally includes the following:
Assessment
At the outset of the initial counseling session, eliciting and addressing the consultand's perceptions and concerns about cancer and his or her expectations of the risk assessment process helps to engage the consultand in the session. This also helps inform the provider about practical or psychosocial issues and guides the focus of counseling and strategies for risk assessment.
Psychosocial assessment
The counseling process that takes place as part of a cancer risk assessment can identify factors that contribute to the consultand's perception of cancer risk and motivations to seek cancer risk assessment and genetic testing. It can also identify potential psychological issues that may need to be addressed during or after the session, particularly after genetic testing. Information collected before and/or during the session may include the following:
Either alone or in consultation with a mental health provider, health care providers offering cancer risk counseling attempt to assess whether there are factors suggesting risk of adverse psychological outcomes after disclosure of risk and/or genetic status.
Clinical Evaluation
Personal health history
Consideration of the consultand's personal health history is essential in cancer risk assessment, regardless of whether the individual has a personal history of cancer. Important information to obtain about the consultand's health history includes the following:[ 1 ][ 3 ]
For consultands with a history of cancer, additional information collected includes the following:
Physical examination
In some cases, a physical exam is conducted by a qualified medical professional to determine whether the individual has physical findings suggestive of a hereditary cancer predisposition syndrome or to rule out evidence of an existing malignancy. For example, a medical professional may look for the sebaceous adenomas seen in Muir-Torre syndrome, measure the head circumference or perform a skin exam to rule out benign cutaneous features associated with Cowden syndrome, or perform a clinical breast and axillary lymph node exam on a woman undergoing a breast cancer risk assessment.
Family history
Documenting the family history
The family history is an essential tool for cancer risk assessment. The family history can be obtained via interview or written self-report; both were found to result in equivalent information.[ 10 ] Studies suggest that paper-based family history questionnaires completed before the appointment provide accurate family history information [ 11 ] and that the use of these questionnaires is an acceptable and understandable family history collection method.[ 12 ] Both multimedia-based (e.g., Internet) and print-based (e.g., family history questionnaires) tools are currently available to gather information about family history. However, on average, print-based tools have been found to be written at lower reading grade levels than multimedia-based tools.[ 13 ] It has been reported that questionnaire-based assessments may lead to some underreporting of family history; therefore, a follow-up interview to confirm the reported information and to capture all relevant family history information may be required.[ 14 ] Collecting family history from multiple relatives in a single family has been shown to increase the number of family members reported to have cancer, compared with family history information provided by a single family member.[ 15 ]
Details of the family health history are best summarized in the form of a family tree, or pedigree. The pedigree, a standardized graphic representation of family relationships, facilitates identification of patterns of disease transmission, recognition of the clinical characteristics associated with specific hereditary cancer syndromes, and determination of the best strategies and tools for risk assessment.[ 16 ][ 17 ]
Standards of pedigree nomenclature have been established.[ 16 ][ 17 ] Refer to Figure 1 for common pedigree symbols.

Figure 1. Standard pedigree nomenclature. Common symbols are used to draw a pedigree (family tree). A pedigree shows relationships between family members and patterns of inheritance for certain traits and diseases. Refer to the paragraph below for descriptions of factors suggesting inherited cancer risk.
Documentation of a comprehensive family cancer history typically includes the following:
A three-generation family history includes the following:
For any relative with cancer, collect the following information:[ 19 ]
For relatives not affected with cancer, collect the following information:
Accuracy of the family history
The accuracy of the family history has a direct bearing on determining the differential diagnoses, selecting appropriate testing, interpreting results of the genetic tests, refining individual cancer risk estimates, and outlining screening and risk reduction recommendations. In a telephone survey of 1,019 individuals, only 6% did not know whether a first-degree relative had cancer; this increased to 8.5% for second-degree relatives.[ 20 ] However, people often have incomplete or inaccurate information about the cancer history in their family.[ 17 ][ 19 ][ 21 ][ 22 ][ 23 ][ 24 ][ 25 ][ 26 ][ 27 ] Patient education has been shown to improve the completeness of family history collection and may lead to more-accurate risk stratification, referrals for genetic counseling, and changes to management recommendations.[ 28 ] Confirming the primary site of cancers in the family that will affect the calculation of hereditary predisposition probabilities and/or estimation of empiric cancer risks may be important, especially if decisions about treatments such as risk-reducing surgery will be based on this family history.[ 23 ][ 29 ]
Accuracy varies by cancer site and degree of relatedness.[ 25 ][ 30 ][ 31 ] Reporting of cancer family histories may be most accurate for breast cancer [ 25 ][ 31 ] and less accurate for gynecologic malignancies [ 25 ][ 31 ] and colon cancer.[ 25 ] Self-reported family histories may contain errors and, in rare instances, could be fictitious.[ 23 ][ 29 ][ 31 ] The most reliable documentation of cancer histology is the pathology report. Verification of cancers can also be made through other medical records, tumor registries, or death certificates.
Determining Cancer Risk
Analysis of the family history
Because a family history of cancer is one of the important predictors of cancer risk, analysis of the pedigree constitutes an important aspect of risk assessment. This analysis might be thought of as a series of the following questions:
-
What is the evidence that a cancer susceptibility syndrome is present in
this family?
The clues to a hereditary syndrome are based on pedigree analysis and physical findings. The index of suspicion is raised by the following:[ 18 ]
Clinical characteristics associated with different cancer genetic syndromes are summarized in the following comprehensive set of personal and family history criteria published by the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors.[ 32 ] These practice guidelines take into account tumor types or other features and related criteria that would indicate a need for a genetics referral. The authors state that the guidelines are intended to maximize appropriate referral of at-risk individuals for cancer genetic consultation but are not meant to provide genetic testing or treatment recommendations.
-
If a syndrome is suspected, what are the differential diagnoses?
The most commonly encountered indications for genetic counseling/testing are for suspected hereditary breast cancer or hereditary colon cancer syndromes.
For hereditary breast cancer, genetic counseling and testing criteria are broad.[ 32 ][ 33 ] Multigene panel testing has revealed that pathogenic variants in several other high- and moderate-penetrance genes other than BRCA1 and BRCA2 contribute to this phenotype, such as PALB2, CHEK2, and ATM.
For hereditary colon cancer syndromes, differential diagnoses are based on several factors, including the number and type of colorectal polyps and histopathology of gastrointestinal and other malignancies.[ 34 ][ 35 ] However, in the absence of polyposis and rare pathologies, Lynch syndrome is frequently in the differential. Furthermore, Lynch syndrome may be in the differential diagnoses list even when there are cases of breast and/or ovarian cancer in the family that are not consistent with hereditary breast and ovarian cancer.[ 36 ][ 37 ] (Refer to the Lynch syndrome section in the PDQ summary on Genetics of Colorectal Cancer for more information.)
Diagnostic and testing criteria exist for several rare syndromes such as Li-Fraumeni,[ 38 ] Cowden,[ 39 ][ 40 ] multiple endocrine neoplasias,[ 41 ] and familial adenomatous polyposis.[ 34 ] In some cases, pathognomonic features are also an indicator for a likely diagnosis.[ 39 ][ 40 ]
Based on these considerations, genetic testing options may consist of limited targeted testing for pathogenic variants in one or a small number of genes, or may consist of larger gene panels.
-
What could make the family history difficult to interpret?
Other factors may complicate recognition of basic inheritance patterns or represent different types of disease etiology.[ 42 ][ 43 ][ 44 ]
Common examples of complicating factors related to family history structure include the following:
Genetic factors that may affect family history interpretation include:
-
What is the most likely mode of inheritance, regardless of whether a
syndrome diagnosis can be established?
The mode of inheritance refers to the way that genetic traits are transmitted in the family.
Most commonly, inheritance patterns are established by a combination of clinical diagnosis with a compatible, but not necessarily in itself conclusive, pedigree pattern.[ 45 ] Most recognized hereditary cancer syndromes are autosomal dominant or autosomal recessive. Clues to recognizing these patterns within a pedigree are described below. (Refer to question 3, What could make the family history difficult to interpret?, for a list of situations that may complicate pedigree interpretation.)
-
What is the chance of a member of this family developing cancer, if an inherited susceptibility
exists?
These probabilities vary by syndrome, family, gene, and pathogenic variant, with different variants in the same gene sometimes conferring different cancer risks, or the same variant being associated with different clinical manifestations in different families. These phenomena relate to issues such as penetrance and expressivity that are discussed elsewhere.
-
If no recognizable syndrome is present, is there a risk of cancer based on other
epidemiological risk factors?
A positive family history may sometimes provide risk information in the absence of a specific genetically determined cancer syndrome. For example, the risk associated with having a single affected relative with breast or colorectal cancer can be estimated from data derived from epidemiologic and family studies. Examples of empiric risk estimates of this kind are provided in the PDQ summaries on Genetics of Breast and Gynecologic Cancers and Genetics of Colorectal Cancer.
Methods of quantifying cancer risk
The overarching goal of cancer risk assessment is to individualize cancer risk management recommendations based on personalized risk. Methods to calculate risk utilize health history information and risk factor and family history data often in combination with emerging biologic and genetic/genomic evidence to establish predictions.[ 48 ] Multiple methodologies are used to calculate risk, including statistical models, prevalence data from specific populations, penetrance data when a documented pathogenic variant has been identified in a family, mendelian inheritance, and Bayesian analysis. All models have distinct capabilities, weaknesses, and limitations based on the methodology, sample size, and/or population used to create the model. Methods to individually quantify risk encompass two primary areas: the probability of harboring a pathogenic variant in a cancer susceptibility gene and the risk of developing a specific form of cancer.[ 48 ]
Risk of harboring a pathogenic variant in a cancer susceptibility gene
The decision to offer genetic testing for cancer susceptibility is complex and can be aided in part by objectively assessing an individual's and/or family's probability of harboring a pathogenic variant.[ 49 ] Predicting the probability of harboring a pathogenic variant in a cancer susceptibility gene can be done using several strategies, including empiric data, statistical models, population prevalence data, Mendel’s laws, Bayesian analysis, and specific health information, such as tumor-specific features.[ 49 ][ 50 ] All of these methods are gene specific or cancer-syndrome specific and are employed only after a thorough assessment has been completed and genetic differential diagnoses have been established.
If a gene or hereditary cancer syndrome is suspected, models specific to that disorder can be used to determine whether genetic testing may be informative. (Refer to the PDQ summaries on the Genetics of Breast and Gynecologic Cancers; Genetics of Colorectal Cancer; or the Genetics of Skin Cancer for more information about cancer syndrome-specific probability models.) The key to using specific models or prevalence data is to apply the model or statistics only in the population best suited for its use. For instance, a model or prevalence data derived from a population study of individuals older than 35 years may not accurately be applied in a population aged 35 years and younger. Care must be taken when interpreting the data obtained from various risk models because they differ with regard to what is actually being estimated. Some models estimate the risk of a pathogenic variant being present in the family; others estimate the risk of a pathogenic variant being present in the individual being counseled. Some models estimate the risk of specific cancers developing in an individual, while others estimate more than one of the data above. (Refer to NCI's Risk Prediction Models website or the disease-specific PDQ cancer genetics summaries for more information about specific cancer risk prediction and pathogenic variant probability models.) Other important considerations include critical family constructs, which can significantly impact model reliability, such as small family size or male-dominated families when the cancer risks are predominantly female in origin, adoption, and early deaths from other causes.[ 42 ][ 50 ] In addition, most models provide gene and/or syndrome-specific probabilities but do not account for the possibility that the personal and/or family history of cancer may be conferred by an as-yet-unidentified cancer susceptibility gene.[ 43 ] In the absence of a documented pathogenic variant in the family, critical assessment of the personal and family history is essential in determining the usefulness and limitations of probability estimates used to aid in the decisions regarding indications for genetic testing.[ 43 ][ 49 ][ 50 ]
When a pathogenic variant has been identified in a family and a test report documents that finding, prior probabilities can be ascertained with a greater degree of reliability. In this setting, probabilities can be calculated based on the pattern of inheritance associated with the gene in which the pathogenic variant has been identified. In addition, critical to the application of mendelian inheritance is the consideration of integrating Bayes Theorem, which incorporates other variables, such as current age, into the calculation for a more accurate posterior probability.[ 1 ][ 51 ] This is especially useful in individuals who have lived to be older than the age at which cancer is likely to develop based on the pathogenic variant identified in their family and therefore have a lower likelihood of harboring the family pathogenic variant when compared with the probability based on their relationship to the carrier in the family.
Even in the case of a documented pathogenic variant on one side of the family, careful assessment and evaluation of the individual’s personal and family history of cancer is essential to rule out cancer risk or suspicion of a cancer susceptibility gene pathogenic variant on the other side of the family (maternal or paternal, as applicable).[ 52 ] Segregation of more than one pathogenic variant in a family is possible (e.g., in circumstances in which a cancer syndrome has founder pathogenic variants associated with families of particular ancestral origin).
Risk of developing cancer
Unlike pathogenic variant probability models that predict the likelihood that a given personal and/or family history of cancer could be associated with a pathogenic variant in a specific gene(s), other methods and models can be used to estimate the risk of developing cancer over time. Similar to pathogenic variant probability assessments, cancer risk calculations are also complex and necessitate a detailed health history and family history. In the presence of a documented pathogenic variant, cancer risk estimates can be derived from peer-reviewed penetrance data.[ 1 ] Penetrance data are constantly being refined and many genetic variants have variable penetrance because other variables may impact the absolute risk of cancer in any given patient. Modifiers of cancer risk in carriers of pathogenic variants include the variant's effect on the function of the gene/protein (e.g., variant type and position), the contributions of modifier genes, and personal and environmental factors (e.g., the impact of bilateral salpingo-oophorectomy performed for other indications in a woman who harbors a BRCA pathogenic variant).[ 53 ] When there is evidence of an inherited susceptibility to cancer but genetic testing has not been performed, analysis of the pedigree can be used to estimate cancer risk. This type of calculation uses the probability the individual harbors a genetic variant and variant-specific penetrance data to calculate cancer risk.[ 1 ]
In the absence of evidence of a hereditary cancer syndrome, several methods can be utilized to estimate cancer risk. Relative risk data from studies of specific risk factors provide ratios of observed versus expected cancers associated with a given risk factor. However, utilizing relative risk data for individualized risk assessment can have significant limitations: relative risk calculations will differ based on the type of control group and other study-associated biases, and comparability across studies can vary widely.[ 51 ] In addition, relative risks are lifetime ratios and do not provide age-specific calculations, nor can the relative risk be multiplied by population risk to provide an individual's risk estimate.[ 51 ][ 54 ]
In spite of these limitations, disease-specific cumulative risk estimates are most often employed in clinical settings. These estimates usually provide risk for a given time interval and can be anchored to cumulative risks of other health conditions in a given population (e.g., the 5-year risk by the Gail model).[ 51 ][ 54 ] Cumulative risk models have limitations that may underestimate or overestimate risk. For example, the Gail model excludes paternal family histories of breast cancer.[ 50 ] Furthermore, many of these models were constructed from data derived from predominantly white populations and may have limited validity when used to estimate risk in other ethnicities.[ 55 ]
Cumulative risk estimates are best used when evidence of other underlying significant risk factors have been ruled out. Careful evaluation of an individual's personal health and family history can identify other confounding risk factors that may outweigh a risk estimate derived from a cumulative risk model. For example, a woman with a prior biopsy showing lobular carcinoma in situ (LCIS) whose mother was diagnosed with breast cancer at age 65 years has a greater lifetime risk from her history of LCIS than her cumulative lifetime risk of breast cancer based on one first-degree relative.[ 56 ][ 57 ] In this circumstance, recommendations for cancer risk management would be based on the risk associated with her LCIS. Unfortunately, there is no reliable method for combining all of an individual's relevant risk factors for an accurate absolute cancer risk estimate, nor are individual risk factors additive.
In summary, careful ascertainment and review of personal health and cancer family history are essential adjuncts to the use of prior probability models and cancer risk assessment models to assure that critical elements influencing risk calculations are considered.[ 49 ] Influencing factors include the following:
A number of investigators are developing health care provider decision support tools such as the Genetic Risk Assessment on the Internet with Decision Support (GRAIDS),[ 58 ] but at this time, clinical judgment remains a key component of any prior probability or absolute cancer risk estimation.[ 49 ]
参考文献- Riley BD, Culver JO, Skrzynia C, et al.: Essential elements of genetic cancer risk assessment, counseling, and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns 21 (2): 151-61, 2012.[PUBMED Abstract]
- Robson ME, Bradbury AR, Arun B, et al.: American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. J Clin Oncol 33 (31): 3660-7, 2015.[PUBMED Abstract]
- Berliner JL, Fay AM, Cummings SA, et al.: NSGC practice guideline: risk assessment and genetic counseling for hereditary breast and ovarian cancer. J Genet Couns 22 (2): 155-63, 2013.[PUBMED Abstract]
- Lancaster JM, Powell CB, Chen LM, et al.: Society of Gynecologic Oncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol 136 (1): 3-7, 2015.[PUBMED Abstract]
- Committee on Practice Bulletins–Gynecology, Committee on Genetics, Society of Gynecologic Oncology: Practice Bulletin No 182: Hereditary Breast and Ovarian Cancer Syndrome. Obstet Gynecol 130 (3): e110-e126, 2017.[PUBMED Abstract]
- Rimer BK, Schildkraut JM, Lerman C, et al.: Participation in a women's breast cancer risk counseling trial. Who participates? Who declines? High Risk Breast Cancer Consortium. Cancer 77 (11): 2348-55, 1996.[PUBMED Abstract]
- Evans DG, Burnell LD, Hopwood P, et al.: Perception of risk in women with a family history of breast cancer. Br J Cancer 67 (3): 612-4, 1993.[PUBMED Abstract]
- Kash KM, Holland JC, Halper MS, et al.: Psychological distress and surveillance behaviors of women with a family history of breast cancer. J Natl Cancer Inst 84 (1): 24-30, 1992.[PUBMED Abstract]
- Davis S, Stewart S, Bloom J: Increasing the accuracy of perceived breast cancer risk: results from a randomized trial with Cancer Information Service callers. Prev Med 39 (1): 64-73, 2004.[PUBMED Abstract]
- Kelly KM, Shedlosky-Shoemaker R, Porter K, et al.: Cancer family history reporting: impact of method and psychosocial factors. J Genet Couns 16 (3): 373-82, 2007.[PUBMED Abstract]
- Armel SR, McCuaig J, Finch A, et al.: The effectiveness of family history questionnaires in cancer genetic counseling. J Genet Couns 18 (4): 366-78, 2009.[PUBMED Abstract]
- Appleby-Tagoe JH, Foulkes WD, Palma L: Reading between the lines: a comparison of responders and non-responders to a family history questionnaire and implications for cancer genetic counselling. J Genet Couns 21 (2): 273-91, 2012.[PUBMED Abstract]
- Wang C, Gallo RE, Fleisher L, et al.: Literacy assessment of family health history tools for public health prevention. Public Health Genomics 14 (4-5): 222-37, 2011.[PUBMED Abstract]
- Vogel TJ, Stoops K, Bennett RL, et al.: A self-administered family history questionnaire improves identification of women who warrant referral to genetic counseling for hereditary cancer risk. Gynecol Oncol 125 (3): 693-8, 2012.[PUBMED Abstract]
- Tehranifar P, Wu HC, Shriver T, et al.: Validation of family cancer history data in high-risk families: the influence of cancer site, ethnicity, kinship degree, and multiple family reporters. Am J Epidemiol 181 (3): 204-12, 2015.[PUBMED Abstract]
- Bennett RL, Steinhaus KA, Uhrich SB, et al.: Recommendations for standardized human pedigree nomenclature. Pedigree Standardization Task Force of the National Society of Genetic Counselors. Am J Hum Genet 56 (3): 745-52, 1995.[PUBMED Abstract]
- Bennett RL, French KS, Resta RG, et al.: Standardized human pedigree nomenclature: update and assessment of the recommendations of the National Society of Genetic Counselors. J Genet Couns 17 (5): 424-33, 2008.[PUBMED Abstract]
- Lu KH, Wood ME, Daniels M, et al.: American Society of Clinical Oncology Expert Statement: collection and use of a cancer family history for oncology providers. J Clin Oncol 32 (8): 833-40, 2014.[PUBMED Abstract]
- Schneider K: Collection and interpretation of cancer histories. In: Schneider KA: Counseling About Cancer: Strategies for Genetic Counseling. 2nd ed. New York, NY: Wiley-Liss, 2002, pp 129-166.[PUBMED Abstract]
- Wideroff L, Garceau AO, Greene MH, et al.: Coherence and completeness of population-based family cancer reports. Cancer Epidemiol Biomarkers Prev 19 (3): 799-810, 2010.[PUBMED Abstract]
- Mitchell RJ, Brewster D, Campbell H, et al.: Accuracy of reporting of family history of colorectal cancer. Gut 53 (2): 291-5, 2004.[PUBMED Abstract]
- Schneider KA, DiGianni LM, Patenaude AF, et al.: Accuracy of cancer family histories: comparison of two breast cancer syndromes. Genet Test 8 (3): 222-8, 2004.[PUBMED Abstract]
- Douglas FS, O'Dair LC, Robinson M, et al.: The accuracy of diagnoses as reported in families with cancer: a retrospective study. J Med Genet 36 (4): 309-12, 1999.[PUBMED Abstract]
- Sijmons RH, Boonstra AE, Reefhuis J, et al.: Accuracy of family history of cancer: clinical genetic implications. Eur J Hum Genet 8 (3): 181-6, 2000.[PUBMED Abstract]
- Mai PL, Garceau AO, Graubard BI, et al.: Confirmation of family cancer history reported in a population-based survey. J Natl Cancer Inst 103 (10): 788-97, 2011.[PUBMED Abstract]
- Ozanne EM, O'Connell A, Bouzan C, et al.: Bias in the reporting of family history: implications for clinical care. J Genet Couns 21 (4): 547-56, 2012.[PUBMED Abstract]
- Brennan P, Claber O, Brennan T: Cancer family history triage: a key step in the decision to offer screening and genetic testing. Fam Cancer 12 (3): 497-502, 2013.[PUBMED Abstract]
- Beadles CA, Ryanne Wu R, Himmel T, et al.: Providing patient education: impact on quantity and quality of family health history collection. Fam Cancer 13 (2): 325-32, 2014.[PUBMED Abstract]
- Evans DG, Kerr B, Cade D, et al.: Fictitious breast cancer family history. Lancet 348 (9033): 1034, 1996.[PUBMED Abstract]
- Qureshi N, Wilson B, Santaguida P, et al.: Collection and Use of Cancer Family History in Primary Care. Evidence Report/Technology Assessment No. 159. Rockville,Md: Agency for Healthcare Research and Quality, 2007. AHRQ Pub No. 08-E001.[PUBMED Abstract]
- Murff HJ, Spigel DR, Syngal S: Does this patient have a family history of cancer? An evidence-based analysis of the accuracy of family cancer history. JAMA 292 (12): 1480-9, 2004.[PUBMED Abstract]
- Hampel H, Bennett RL, Buchanan A, et al.: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 17 (1): 70-87, 2015.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 1.2020. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed December 23, 2019.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal. Version 3.2019. Plymouth Meeting, PA: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed February 05, 2020.[PUBMED Abstract]
- Spoto CPE, Gullo I, Carneiro F, et al.: Hereditary gastrointestinal carcinomas and their precursors: An algorithm for genetic testing. Semin Diagn Pathol 35 (3): 170-183, 2018.[PUBMED Abstract]
- Roberts ME, Jackson SA, Susswein LR, et al.: MSH6 and PMS2 germ-line pathogenic variants implicated in Lynch syndrome are associated with breast cancer. Genet Med 20 (10): 1167-1174, 2018.[PUBMED Abstract]
- Espenschied CR, LaDuca H, Li S, et al.: Multigene Panel Testing Provides a New Perspective on Lynch Syndrome. J Clin Oncol 35 (22): 2568-2575, 2017.[PUBMED Abstract]
- Bougeard G, Renaux-Petel M, Flaman JM, et al.: Revisiting Li-Fraumeni Syndrome From TP53 Mutation Carriers. J Clin Oncol 33 (21): 2345-52, 2015.[PUBMED Abstract]
- Pilarski R, Eng C: Will the real Cowden syndrome please stand up (again)? Expanding mutational and clinical spectra of the PTEN hamartoma tumour syndrome. J Med Genet 41 (5): 323-6, 2004.[PUBMED Abstract]
- Eng C: PTEN Hamartoma Tumor Syndrome (PHTS). In: Pagon RA, Adam MP, Bird TD, et al., eds.: GeneReviews. Seattle, Wash: University of Washington, 1993-2018, pp. Available online. Last accessed December 19, 2019.[PUBMED Abstract]
- Brandi ML, Gagel RF, Angeli A, et al.: Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab 86 (12): 5658-71, 2001.[PUBMED Abstract]
- Weitzel JN, Lagos VI, Cullinane CA, et al.: Limited family structure and BRCA gene mutation status in single cases of breast cancer. JAMA 297 (23): 2587-95, 2007.[PUBMED Abstract]
- Kauff ND, Offit K: Modeling genetic risk of breast cancer. JAMA 297 (23): 2637-9, 2007.[PUBMED Abstract]
- Kramer JL, Velazquez IA, Chen BE, et al.: Prophylactic oophorectomy reduces breast cancer penetrance during prospective, long-term follow-up of BRCA1 mutation carriers. J Clin Oncol 23 (34): 8629-35, 2005.[PUBMED Abstract]
- Harper PS: Practical Genetic Counselling. 3rd ed. London: Wright, 1988.[PUBMED Abstract]
- Whitworth J, Skytte AB, Sunde L, et al.: Multilocus Inherited Neoplasia Alleles Syndrome: A Case Series and Review. JAMA Oncol 2 (3): 373-9, 2016.[PUBMED Abstract]
- Stratton MR: Exploring the genomes of cancer cells: progress and promise. Science 331 (6024): 1553-8, 2011.[PUBMED Abstract]
- Freedman AN, Seminara D, Gail MH, et al.: Cancer risk prediction models: a workshop on development, evaluation, and application. J Natl Cancer Inst 97 (10): 715-23, 2005.[PUBMED Abstract]
- Lindor NM, Lindor RA, Apicella C, et al.: Predicting BRCA1 and BRCA2 gene mutation carriers: comparison of LAMBDA, BRCAPRO, Myriad II, and modified Couch models. Fam Cancer 6 (4): 473-82, 2007.[PUBMED Abstract]
- Domchek SM, Eisen A, Calzone K, et al.: Application of breast cancer risk prediction models in clinical practice. J Clin Oncol 21 (4): 593-601, 2003.[PUBMED Abstract]
- Offit K, Brown K: Quantitating familial cancer risk: a resource for clinical oncologists. J Clin Oncol 12 (8): 1724-36, 1994.[PUBMED Abstract]
- Apicella C, Andrews L, Hodgson SV, et al.: Log odds of carrying an Ancestral Mutation in BRCA1 or BRCA2 for a Defined personal and family history in an Ashkenazi Jewish woman (LAMBDA). Breast Cancer Res 5 (6): R206-16, 2003.[PUBMED Abstract]
- Chenevix-Trench G, Milne RL, Antoniou AC, et al.: An international initiative to identify genetic modifiers of cancer risk in BRCA1 and BRCA2 mutation carriers: the Consortium of Investigators of Modifiers of BRCA1 and BRCA2 (CIMBA). Breast Cancer Res 9 (2): 104, 2007.[PUBMED Abstract]
- Hoskins KF, Stopfer JE, Calzone KA, et al.: Assessment and counseling for women with a family history of breast cancer. A guide for clinicians. JAMA 273 (7): 577-85, 1995.[PUBMED Abstract]
- Adams-Campbell LL, Makambi KH, Palmer JR, et al.: Diagnostic accuracy of the Gail model in the Black Women's Health Study. Breast J 13 (4): 332-6, 2007 Jul-Aug.[PUBMED Abstract]
- Fisher ER, Land SR, Fisher B, et al.: Pathologic findings from the National Surgical Adjuvant Breast and Bowel Project: twelve-year observations concerning lobular carcinoma in situ. Cancer 100 (2): 238-44, 2004.[PUBMED Abstract]
- Chuba PJ, Hamre MR, Yap J, et al.: Bilateral risk for subsequent breast cancer after lobular carcinoma-in-situ: analysis of surveillance, epidemiology, and end results data. J Clin Oncol 23 (24): 5534-41, 2005.[PUBMED Abstract]
- Emery J, Morris H, Goodchild R, et al.: The GRAIDS Trial: a cluster randomised controlled trial of computer decision support for the management of familial cancer risk in primary care. Br J Cancer 97 (4): 486-93, 2007.[PUBMED Abstract]
-
What is the evidence that a cancer susceptibility syndrome is present in
this family?
- The Option of Genetic Testing
-
Factors to Consider When Offering Testing
Indications for testing
Experts recommend offering genetic testing when a risk assessment suggests the presence of an inherited cancer syndrome for which specific genes have been identified. The American Society of Clinical Oncology (ASCO) Policy Statement on Genetic Testing for Cancer Susceptibility proposes that genetic testing be offered when the following conditions apply:[ 1 ][ 2 ]
Characteristics used in making this determination are discussed in the PDQ summaries on the genetics of specific cancers. Even when individual and family history characteristics indicate a possible inherited cancer syndrome, individuals may elect not to proceed with testing after discussion of potential risks, benefits, and limitations, as discussed below. Conversely, individuals whose pedigrees are incomplete or uninformative due to very small family size, early deaths, or incomplete data on key family members may elect to pursue genetic testing in an attempt to better define their risk status. In these situations, it is particularly important that the pretest counseling fully explore the limitations of the testing process.
ASCO's 2010 and 2015 policy statements addressed testing for low- to moderate-penetrance genes and direct-to-consumer testing.[ 1 ][ 2 ]
ASCO’s position is that when a test, regardless of clinical utility, is ordered by a health care professional, the provider is responsible for organizing follow-up care based on the findings. For tests that are ordered by the consumer without health care professional involvement, management decisions are based on the evidence for clinical utility. For tests with accepted clinical utility, follow-up care can be guided by the evidence for cancer risk associated with the genetic test finding. However, in tests ordered by the consumer that have uncertain clinical utility, ASCO recommends that follow-up care consist of education regarding the lack of evidence regarding the test's clinical utility and that cancer risk management decisions be guided by established cancer risk factors.[ 1 ][ 2 ]
In 2015, ASCO updated its policy to address the challenges of new technologies in cancer genetics, including multigene (panel) testing for cancer genetic susceptibility, as well as incidental germline findings from somatic mutation profiling.[ 2 ] ASCO's statement expressed support for communicating medically relevant germline findings discovered in the context of somatic mutation profiling.[ 2 ]
Genetic education and counseling, including the interpretation of genetic test results, will vary depending on whether a previous attempt at genetic testing has been made (refer to Figure 2). In general, there are two primary circumstances in which genetic testing is performed:
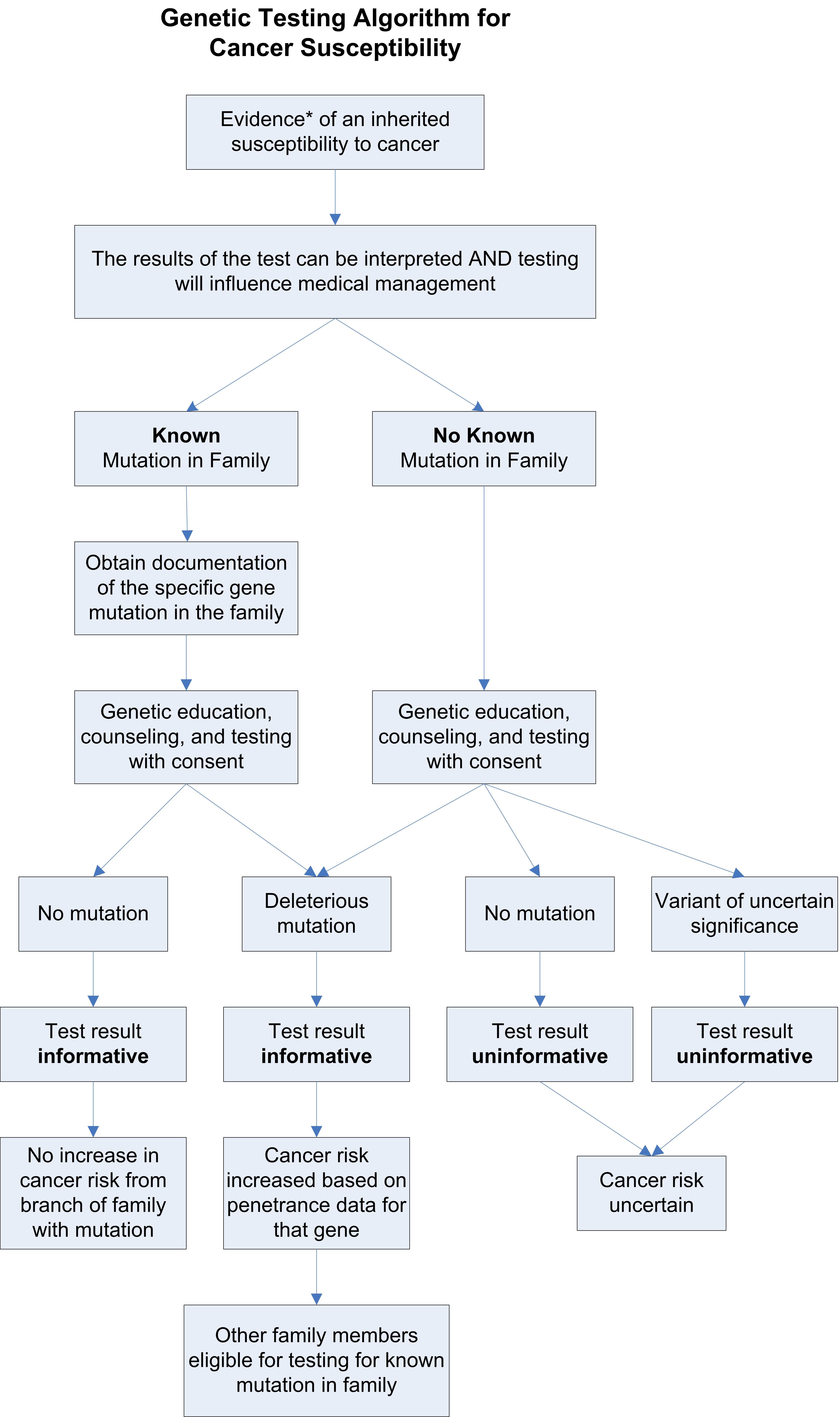
Figure 2. This genetic testing algorithm depicts the multistep process of testing for cancer susceptibility. Value of testing an affected family member first
Genetic susceptibility testing generally yields the most useful information when a living family member affected with the cancer of concern is tested first to determine whether a genetic basis for the cancer diagnosis can be established. If testing is deferred while follow-up with an affected relative is pending, consider providing interim cancer risk management guidelines to the unaffected proband.[ 3 ] Three possible outcomes of testing include the following (refer to Figure 2):
If a documented pathogenic variant (associated with cancer risk) is identified, risks are based on penetrance data for pathogenic variants of that specific gene. In addition, other family members may be tested for the presence or absence of this specific pathogenic variant. If no variant is found in an affected family member, testing is considered uninformative and thus there is no basis for testing unaffected relatives. Failure of the laboratory to detect a pathogenic variant in an affected family member does not rule out an inherited basis for the cancer in that family. Reasons why testing could be uninformative include the following:
Lastly, testing may reveal a VUS. This result means that a genetic variant has been found; however, the extent that this variant increases cancer risk, or whether it is associated with the history of cancer in the family, is uncertain. In this circumstance, some clues as to the significance of the variant can be derived from the following:
Unfortunately, even with this information, there is often insufficient evidence to document the significance of a specific variant, and further clarifying research is required.
If there is no close, living, affected relative to undergo testing, or the living affected relative declines testing, other options may be discussed with the patient and the testing laboratory. In rare instances, if proper authorization is secured from the family, testing the stored tissue of a deceased relative may be considered. However, genetic tests done on stored tissue are technically difficult and may not yield a definitive result. Therefore, testing an unaffected person without prior testing of an affected family member may be performed. In these instances, counseling includes discussing that a negative test result does not rule out the presence of a cancer susceptibility gene in the family or in the patient and may be uninformative.
Testing in families with a documented pathogenic variant
Genetic susceptibility testing for a documented pathogenic variant in the family can be very informative and will yield one of the following two results (refer to Figure 2):
If the familial pathogenic variant is detected in a family member, their cancer risks are based on penetrance data for pathogenic variants in that specific gene. If the documented pathogenic variant is not found in a family member, the risk of cancer in that individual is equivalent to cancer risk in the general population. However, other risk factors and family history from the side of the family not associated with the documented pathogenic variant may increase the cancer risk above the general population levels.
In summary, genetic education and counseling includes identifying the most informative person in the family to test, which may be an affected family member rather than the individual seeking genetic services. In addition, counseling includes a discussion of the limitations of the test, all possible test outcomes, and the consequences of identifying a VUS.[ 4 ]
Insurance coverage
Insurance coverage varies for cancer susceptibility testing, including multigene (panel) testing. In general, most individuals who meet specific criteria (e.g., National Comprehensive Cancer Network [NCCN] guidelines for BRCA1/BRCA2 or Lynch syndrome testing) are able to obtain insurance coverage for multigene testing.[ 5 ] Of note, some insurance companies have contracts with specific laboratories through which testing must be ordered.
The Affordable Care Act (ACA) requires that private insurers cover—with no out-of-pocket costs to the insured—genetic counseling and BRCA1/BRCA2 testing for unaffected women meeting United States Preventive Services Task Force guidelines.[ 6 ][ 7 ] Importantly, under ACA guidelines, women with a prior cancer diagnosis are not covered. The ACA does not stipulate that follow-up care based on genetic test results be covered (e.g., risk-reducing surgeries). However, some insurance companies require that pretest genetic counseling be performed by a credentialed genetics provider before testing is authorized. Before testing is ordered, it is important to verify costs and insurance coverage, including for Medicaid and Medicare patients. Medicare does not cover genetic testing if the patient has not had a cancer diagnosis associated with the pathogenic variants for which testing is ordered. In addition, unaffected individuals with Medicare are not covered for testing, even if they are tested for only a known familial pathogenic variant. Further, Medicare does not cover genetic counseling as a separately billable service.[ 8 ] For individuals without insurance coverage and the underinsured, some laboratories offer low-cost options or have financial assistance programs.
Genetic testing and assisted reproductive technology
There is a risk of carriers passing on cancer-associated pathogenic variants to offspring. When an individual tests positive for one pathogenic variant in a cancer susceptibility gene, counseling about reproductive implications addresses not only the risks associated with autosomal dominant inheritance but also the potential risks of having a child with two pathogenic variants in the same gene (biallelic) that could result in a severe condition.
Assisted reproductive technology can be used for preimplantation genetic testing (PGT) and for prenatal cancer predisposition genetic testing using chorionic villus sampling and amniocentesis.[ 9 ][ 10 ][ 11 ] For individuals with autosomal dominant cancer syndromes (e.g., those associated with APC, BRCA1/BRCA2, PTEN, or TP53 pathogenic variants), reproductive options exist for prenatal testing and PGT to detect offspring with one copy of the pathogenic variant (heterozygotes).
In some cases (e.g., carriers of germline pathogenic variants in ATM, BLM), assessing an individual’s partner's risk for carrying a pathogenic variant associated with a dominant or recessive syndrome (i.e., his or her personal and family history and ethnicity) is indicated. In the unlikely event that both parents are heterozygous for specific pathogenic variants, there is a 25% risk that a child will be homozygous and could have a severe phenotype. In light of this information, couples may consider PGT or prenatal testing.
A proposed analytic framework for counseling carriers about reproduction options includes consideration of the following issues:[ 10 ]
- Does the cancer syndrome include childhood malignancies or significant morbidity or mortality at an early age?
- What is the penetrance associated with the genetic variant?
- How severe is the syndrome phenotype?
- Are there interventions available that decrease the pathogenic variant-associated cancer risk or are proven to detect cancer early when it is in a treatable form?
- Is there evidence of a different phenotype if an individual is a heterozygous or homozygous carrier?[ 12 ][ 13 ]
In a study of 320 patients with different hereditary cancer syndromes, most were unaware of PGT; however, the majority expressed interest in learning more about the availability of PGT.[ 14 ] Patients also preferred having a discussion about PGT with their genetic counselor or primary physician. Disease-specific factors (e.g., severity of the hereditary condition, quality of life, and medical interventions) and individual factors (e.g., gender, childbearing status, and religious beliefs) affected patient attitudes about PGT.
Determining the Test to Be Used
Genetic testing is highly specialized. There are also multiple molecular testing methods available, each with its own indications, costs, strengths, and weaknesses. Depending on the method employed and the extent of the analysis, different tests for the same gene will have varying levels of sensitivity and specificity. Even assuming high analytic validity, genetic heterogeneity makes test selection challenging. A number of different genetic syndromes may underlie the development of a particular cancer type. For example, hereditary colorectal cancer may be due to familial adenomatous polyposis (FAP), Lynch syndrome, Peutz-Jeghers syndrome, juvenile polyposis syndrome, or other syndromes. Each of these has a different genetic basis. In addition, different genes may be responsible for the same condition (e.g., Lynch syndrome can be caused by pathogenic variants in one of several mismatch repair [MMR] genes).
In some genes, the same pathogenic variant has been found in multiple, apparently unrelated families. This observation is consistent with a founder effect, wherein a pathogenic variant identified in a contemporary population can be traced back to a small group of founders isolated by geographic, cultural, or other factors. For example, two specific BRCA1 pathogenic variants (68_69delAG and 5266dup, also known in the literature as 185delAG and 5382insC) and one BRCA2 pathogenic variant (5946delT, also known as 6174delT) have been reported to be common in Ashkenazi Jews. Other genes also have reported founder pathogenic variants. The presence of founder pathogenic variants has practical implications for genetic testing. Many laboratories offer directed testing specifically for ethnic-specific alleles. This greatly simplifies the technical aspects of the test but is not without limitations. For example, approximately 15% of BRCA1 and BRCA2 pathogenic variants that occur among Ashkenazim are nonfounder pathogenic variants.[ 15 ] Also, for genes in which large genome rearrangements are common in the founder population, ordering additional testing using different techniques may be needed.
Allelic heterogeneity (i.e., different variants within the same gene) can confer different risks or be associated with a different phenotype. For example, though the general rule is that adenomatous polyposis coli (APC) pathogenic variants are associated with hundreds or thousands of colonic polyps and colon cancer of the classical FAP syndrome, some APC pathogenic variants cause a milder clinical picture, with fewer polyps and lower colorectal cancer risk.[ 16 ][ 17 ] In addition, other disorders may be part of the FAP spectrum. Pathogenic variants in a certain portion of the APC gene also predispose to retinal changes, for example, when pathogenic variants in a different region of APC predispose to desmoid tumors.
In light of the heterogeneity in presentation and potential overlap in phenotypes among the various hereditary cancer syndromes, the selection of the appropriate genetic test for a given individual requires knowledge of genetic syndromes, molecular diagnostic methods used for identifying pathogenic variants, correlation between clinical and molecular findings, and access to information about rapidly changing testing options. These issues are addressed in detail in PDQ summaries on the genetics of specific cancers. (Refer to the PDQ summaries on Genetics of Breast and Gynecologic Cancers; Genetics of Colorectal Cancer; Genetics of Endocrine and Neuroendocrine Neoplasias; Genetics of Skin Cancer; Genetics of Kidney Cancer [Renal Cell Cancer]; and Genetics of Prostate Cancer for more information.)
Multigene (panel) testing
Next-generation sequencing (NGS) and the removal of most patent barriers to diagnostic DNA sequencing [ 18 ] have resulted in the availability of multigene testing, which can simultaneously test more than 50 genes for pathogenic variants, often at costs comparable to single-gene testing. These multigene panels can include genes with pathogenic variants that are associated with high risks of cancer and genes that confer moderate and uncertain risks. The multigene panels can be limited to specific cancer types (e.g., breast, ovarian, colon) or can include many cancer types. This type of testing has both advantages and disadvantages, and much of the information presented in this section is not based on empirical data but rather on commentaries.
Genetic education and counseling for multigene testing
ASCO has stressed the importance of genetic counseling to ensure patients are adequately informed about the implications of this type of testing and recommends that tests be ordered by cancer genetic professionals.[ 2 ][ 19 ] Yet, the use of multigene testing requires modification of traditional approaches to genetic counseling.[ 20 ][ 21 ] Optimal evidence-based counseling strategies have not yet been established. Unlike in-person, single-gene pretest genetic counseling models, these approaches have not been examined for outcomes of counseling such as comprehension, satisfaction, psychosocial outcomes, and testing uptake. Table 2 summarizes recommendations from ASCO on elements of pretest genetic counseling and informed consent for germline cancer genetic testing.[ 2 ]
Table 2. Elements of Pretest Genetic Counseling and Informed Consent for Germline Cancer Genetic Testinga Topic Traditional Germline Cancer Genetic Testing Multigene Panel Germline Cancer Genetic Testing aAdapted from Robson et al.[ ] Gene Information Specific gene(s) or gene variant(s) being tested. Review of specific genes included in a multigene panel may need to be batched because it is not feasible to individually cover each gene. Risks associated with the gene(s) or gene variants(s) and implications for health care. Describe high-penetrance gene(s) and/or syndromes included in the multigene panel (i.e., hereditary breast-ovarian syndrome, Lynch syndrome, hereditary diffuse gastric cancer, Li-Fraumeni syndrome), possible detection based on personal and family history and general implications for health care. Describe generally genes of uncertain clinical utility. Possible Test Outcomes • Pathogenic variant detected. • No variant detected. • Variant of uncertain significance (VUS) detected. Variant in a gene for which there is: • Limited evidence regarding penetrance. • Discordant findings (pathogenic variant identified in a gene that is inconsistent with the patient's personal and/or family history). Increased rate of VUS. Risks, Benefits, and Limitations of Genetic Testing Psychosocial implications of test results. Confidentiality considerations, including privacy, data security, and placement of results (i.e., electronic health record). Use of DNA sample(s) for future research. Employment and insurance discrimination risks and protections. Costs involved in testing and scope of insurance coverage if applicable. Whether the genetic health care professional is employed by the testing company. Implications of Genetic Testing for Family Members Pattern of variant transmission and risks of inheritance in children and other family members. Importance of sharing test results with family members. Possible reproductive implications associated with pathogenic variants in genes associated with recessive conditions (i.e., ATM, Fanconi anemia [BRCA2, PALB2], NBN, BLM). Use of Genetic Test Results Implications of genetic test results on health care. Research examining multigene testing
The range of results from NGS multigene panels is emerging in both data from clinical and laboratory series. Several of the studies are collaborations between the two. There are several important caveats about the research that has been conducted so far with regard to multigene testing:
In high-risk individuals who meet criteria for hereditary cancer genetic testing but in whom no pathogenic variant was identified from single-gene testing, panel testing may identify other clinically actionable variants.[ 27 ][ 28 ] For example, the additional yield of multigene testing in individuals in whom a BRCA1/BRCA2 pathogenic variant was not detected currently seems to be approximately 4%.[ 26 ][ 29 ][ 30 ] The most common non-BRCA pathogenic variants found are in CHEK2, ATM, and PALB2.[ 26 ][ 29 ][ 30 ][ 31 ] In some cases, the identification of pathogenic variants from panel testing resulted in additional recommendations for screening and risk reduction beyond what would have been indicated based on family history alone.[ 30 ][ 32 ][ 33 ][ 34 ]
Selected reports from 2014 to 2018, which included 1,000 to 10,000 tested individuals, showed variation in pathogenic variant and VUS rates.[ 23 ][ 24 ][ 26 ][ 30 ][ 35 ][ 36 ][ 37 ][ 38 ] Pathogenic variant rates ranged from 7% to 14%; VUS rates ranged from 19% to 41% and increased with the number of genes included on the panel, but decreased in the later studies, likely because of larger data pools and refinements in variant interpretation. Additionally, VUS rates were higher in non-white individuals, likely because of the limited availability of test result data needed for accurate determination of risk.[ 38 ]
A large study published by a commercial laboratory included more than 252,000 individuals who were tested with a 25-gene panel between 2013 and 2016.[ 39 ] The study reported an overall pathogenic variant rate of 6.7% (9.8% in affected individuals and 4.7% in unaffected individuals), with an overall VUS rate of 30%. The study population was 97% female, had no prior cancer genetic testing, and 93% met NCCN criteria for hereditary breast and ovarian cancer (HBOC) or Lynch syndrome testing. It was noted that half of the pathogenic variants found for HBOC or Lynch syndrome were not in the expected genes associated with these syndromes (BRCA1, BRCA2, MLH1, MSH2, MSH6, and PMS2).
Outcomes of multigene testing
Results from multigene tests have several possible outcomes, including the following:[ 19 ]
Results can also reveal more than one finding given that multiple genes are being tested simultaneously and the elevated rate of VUS.[ 21 ] There has been no assessment of outcomes of multigene tests such as comprehension, psychosocial outcomes, and uptake of cancer risk management options.
Considerations when using multigene testing
Utilizing multigene panels can be complex but may offer advantages over sequential testing strategies. First, in some types of cancer, several genes can be associated with specific phenotypes; therefore, testing for all genes associated with a given phenotype can save both time and money.[ 40 ] Additionally, multigene testing may help identify the genetic basis for cancer in families in whom the differential diagnosis includes multiple syndromes or when the family history does not meet standard criteria for a single cancer syndrome.[ 21 ][ 40 ] (Refer to the Analysis of the family history section of this summary for a list of factors that may make a family history difficult to interpret.)
However, there can be challenges to employing this testing approach. Clinical laboratories now offer a varying array of clinical cancer susceptibility gene panels.[ 41 ][ 42 ] Multigene panels continue to evolve, and the genes included on the panels can change. Other challenges of interpreting multigene test results include higher rates of VUS than with single-gene testing (the rate of VUS increases with the number of genes tested),[ 24 ] higher rates of VUS in some minority populations,[ 32 ][ 43 ] and the detection of variants in genes associated with uncertain cancer risks.
In addition to these primary challenges, providers deciding the optimal testing strategy may also consider the following: the overall expense and out-of-pocket expense to the patient; insurance reimbursement; time frame to complete the test; ease of laboratory use for the clinician ordering testing; the probability of identifying a VUS and management of those findings, such as the reclassification process and provision of supplemental data regarding the variant; technical differences, such as the presence of a deletion/duplication assay; patient preference; and clinical history.[ 2 ][ 40 ][ 41 ][ 44 ]
Overall, there is insufficient evidence to determine superiority of multigene testing over phenotype-guided testing or sequential gene testing.[ 19 ] As a consequence, practice guidelines for optimal clinical use of multigene tests continue to evolve.[ 2 ][ 45 ] The NCCN and ASCO guidelines suggest that efficiencies may be gained by using multigene testing when there is more than one cancer syndrome or gene on the differential diagnosis list.[ 2 ][ 45 ] Additionally, NCCN states that there may be a role for multigene testing when a patient has a personal or family history that is consistent with an inherited susceptibility but single-gene testing has not identified a pathogenic variant.[ 45 ]
Another important consideration is that multigene tests may include genes in which pathogenic variants are associated with moderate or uncertain penetrance. Management of individuals with pathogenic variants in such genes can present additional challenges, particularly when expert consensus or evidence-based recommendations are not available. (Refer to Figure 1 in the Cancer Genetics Overview PDQ summary for information about moderate and low penetrance.) Moreover, there may be limited or no evidence to support changes to medical management based on the level of risk or uncertain risk; however, management may still be affected by family history.[ 1 ][ 2 ] A framework for clinical management incorporates emerging data on age-specific, lifetime, and absolute cancer risks conferred by pathogenic variants in several moderate-risk genes.[ 46 ] (Refer to the Penetrance of Inherited Susceptibility to Hereditary Breast and/or Gynecologic Cancers section in the PDQ summary on Genetics of Breast and Gynecologic Cancers for more information about this framework.)
Regulation of genetic tests
Government regulation of genetic tests to date remains extremely limited in terms of both analytic and clinical validity with little interagency coordination.[ 47 ] The Centers for Medicare & Medicaid Services, using the Clinical Laboratory Improvement Act (CLIA), regulates all clinical human laboratory testing performed in the United States for the purposes of generating diagnostic or other health information. CLIA regulations address personnel qualifications, laboratory quality assurance standards, and documentation and validation of tests and procedures.[ 48 ] For laboratory tests themselves, CLIA categorizes tests based on the level of complexity into waived tests, moderate complexity, or high complexity. Genetic tests are considered high complexity, which indicates that a high degree of knowledge and skill is required to perform or interpret the test. Laboratories conducting high complexity tests must undergo proficiency testing at specified intervals, which consists of an external review of the laboratory's ability to accurately perform and interpret the test.[ 47 ][ 49 ] However, a specialty area specific for molecular and biologic genetic tests has yet to be established; therefore, specific proficiency testing of genetic testing laboratories is not required by CLIA.[ 47 ]
In regard to analytic validity, genetic tests fall into two primary categories; test kits and laboratory-developed tests (previously called home brews). Test kits are manufactured for use in laboratories performing the test and include all the reagents necessary to complete the analysis, instructions, performance outcomes, and details about which genetic variants can be detected. The U.S. Food and Drug Administration (FDA) regulates test kits as medical devices; however, despite more than 1,000 available genetic tests, there are fewer than ten FDA-approved test kits.[ 49 ] Laboratory-developed tests are performed in a laboratory that assembles its own testing materials in-house;[ 49 ] this category represents the most common form of genetic testing. Laboratory-developed tests are subject to the least amount of oversight, as neither CLIA nor the FDA evaluate the laboratories' proficiency in performing the test or clinical validity relative to the accuracy of the test to predict a clinical outcome.[ 47 ][ 49 ] The FDA does regulate manufactured analyte-specific reagents (ASRs) as medical devices. These small molecules are used to conduct laboratory-developed tests but can also be made by the laboratory. ASRs made in the laboratory are not subject to FDA oversight. For laboratory-developed tests utilizing manufactured commercially available ASRs, the FDA requires that the test be ordered by a health professional or other individual authorized to order the test by state law. However, this regulation does not distinguish between health providers caring for the patient or health providers who work for the laboratory offering the test.[ 49 ]
In addition to the regulation of classical clinical genetic tests is the regulatory oversight of research genetic testing. Laboratories performing genetic testing on a research basis are exempt from CLIA oversight if the laboratory does not report patient-specific results for the diagnosis, prevention, or treatment of any disease or impairment or the assessment of the health of individual patients.[ 47 ] However, there are anecdotal reports of research laboratories providing test results for clinical purposes with the caveat that the laboratory recommends that testing be repeated in a clinical CLIA-approved laboratory. In addition, there is no established mechanism that determines when a test has sufficient analytic and clinical validity to be offered clinically.[ 49 ] Currently, the decision to offer a genetic test clinically is at the discretion of the laboratory director.
Evidence regarding the implications of this narrow regulatory oversight of genetic tests is limited and consists predominantly of laboratory director responses to quality assurance surveys. A survey of 133 laboratory directors performing genetic tests found that 88% of laboratories employed one or more American Board of Medical Genetics (ABMG)-certified or ABMG-eligible professional geneticists, and 23% had an affiliation with at least one doctoral-prepared geneticist. Eight percent of laboratories did not employ and were not affiliated with doctoral-level genetics professionals. Laboratory-developed tests were performed in 70% of laboratories. Sixty-three percent of laboratories provided an interpretation of the test result as part of the test report.[ 50 ] Another survey of 190 laboratory directors found that 97% were CLIA-certified for high complexity testing. Sixteen percent of laboratories reported no specialty area certification; those without specialty certification represented laboratories with the most volume of tests performed and offered the most extensive test selection.[ 47 ] Of laboratories with specialty certification, not all had certification relevant to genetic tests, with 48% reporting pathology certification, 46% chemistry certification, and 41% clinical cytogenetics certification. Sixteen percent of directors reported participation in no formal external proficiency testing program, although 77% performed some informal proficiency testing when a formal external proficiency testing program was not available.
The most frequent reason cited for lack of proficiency testing participation was lack of available proficiency testing programs. Laboratory directors estimated that in the past 2 years 37% issued three or fewer incorrect reports, and 35% issued at least four incorrect reports. Analytic errors such as faulty reagent, equipment failure, or human error, increased 40% with each decrease in level of proficiency training completed.[ 47 ] An international genetic testing laboratory director survey involving 18 countries found that 64% of the 827 laboratories that responded accepted samples from outside their country.[ 51 ] Similar to the U.S. study, 74% reported participation in some form of proficiency testing. Fifty-three percent of the laboratories required a copy of the consent to perform the test, and 72% of laboratories retained specimens indefinitely that were submitted for testing.[ 51 ]
The U.S. Department of Health and Human Services Secretary’s Advisory Committee on Genetics, Health, and Society has published a detailed report regarding the adequacy and transparency of the current oversight system for genetic testing in the United States.[ 52 ] The Committee identified gaps in the following areas:
In October 2014, the FDA posted the notification regarding its plans to develop draft guidance on the regulation of laboratory-developed tests.[ 53 ] Draft guidance documents outlining the framework for regulatory oversight for the industry and clinical laboratories were published later in 2014 for public review and comment. Given the potential of such regulatory action to affect the wide spectrum of genetic tests in clinical practice, proposed draft guidelines have been discussed and reviewed by a number of professional associations, eliciting policy statements and analyses from various professional associations, including the American Society of Human Genetics (ASHG) and the Association for Molecular Pathology. The issue of FDA oversight of laboratory-developed tests remains under consideration.
Direct-to-Consumer (DTC) Genetic Tests
Most genetic testing for cancer and other health risks is offered by health care providers on the basis of a patient’s personal history, family history, or ethnicity. Increasingly, however, individuals can order genetic testing through DTC companies without the input of health care providers. DTC tests may provide information about ancestry, paternity, propensity toward certain physical traits, risk of adverse drug reactions, and disease risks.
Genotyping for carrier status and disease risks
In 2015, the FDA provided clearance for a large DTC company (23andMe) to market carrier screening for Bloom syndrome, which is associated with increased cancer risks in homozygotes as well as other phenotypic features. Subsequently, DTC carrier testing for several conditions became available. In 2017, the FDA allowed 23andMe to market DTC tests for ten diseases or conditions including late-onset Alzheimer disease, Parkinson disease, and hereditary thrombophilia.[ 54 ] It is important to note that the carrier and health tests authorized for marketing by the FDA are performed by genotyping, which means that only specific nucleotides or bases are targeted for analysis; sequencing is not performed.[ 55 ] Thus, while the false-positive or false-negative rate for a specific genotype is very low (i.e., analytic validity is high), other pathogenic variants are not analyzed, nor is the entire sequence of the gene. Thus, the false-negative rate due to untested pathogenic variants as well as other gene abnormalities is high.
Genotyping for founder pathogenic variants in BRCA1 and BRCA2
In March 2018, the FDA authorized 23andMe to market DTC testing for three founder pathogenic variants in the BRCA1 and BRCA2 genes that are common in individuals of Ashkenazi Jewish descent.[ 56 ] These three variants are rare among high-risk individuals who are not of this ethnicity and in the general population of non-Jewish individuals. However, Jewish individuals whose family history is suggestive of hereditary breast/ovarian cancer who test negative for these three variants warrant additional testing.
It is crucial for individuals who obtain a BRCA1/BRCA2 (or any health-related) positive result from DTC testing to pursue clinical confirmation of such a result. Clinical confirmation entails repeating the test in a CLIA-certified laboratory, as well as individual review and verification of the result by laboratory personnel.
A potential advantage of DTC testing of these three BRCA1/BRCA2 pathogenic variants is that it will identify individuals who would not have been otherwise aware of their increased risk of associated cancers, for example if they have no personal or family history of breast, ovarian, or prostate cancer. This is one of the main arguments for population-based screening for BRCA1/BRCA2 pathogenic variants. (Refer to the Population screening section in the PDQ summary on Genetics of Breast and Gynecologic Cancers for more information.)
However, a negative result does not rule out other hereditary factors or account for other clinical indicators, genetic and nongenetic, of increased cancer risk. Thus, for most individuals who test negative for the three BRCA1/BRCA2 variants, the results do not provide reassurance about their cancer risks. For high-risk individuals in particular (i.e., those with a history suggestive of hereditary breast/ovarian cancer) a negative result from this limited testing is incomplete, given that it does not assess the presence or absence of other pathogenic variants in BRCA1/BRCA2 or in many other cancer-associated genes.
Consumer-directed clinical testing
Consumer-directed clinical testing is used to describe a hybrid approach to genetic testing, whereupon clinical–grade genetic testing can be initiated and selected by a consumer; however, ordering of the test by an authorized provider (e.g., primary care physician, nurse practitioner, or genetic counselor) is required.[ 57 ] The test ordering may be coordinated by the testing company. Genetic counseling may also be offered by the laboratory to explain the results.
With respect to cancer genetic testing, there are clinical, CLIA-certified laboratories that offer multigene (panel) tests as a consumer-directed service. Things to consider when genetic testing is ordered this way include:
-
Is the test the same as what would have been ordered by the individual’s own health care provider after review of personal and family history?
Multigene (panel) tests may not include all high- to moderate-risk genes in the differential, or newer/preliminary evidence genes.
-
Are variants of uncertain significance (VUS) reported back to the consumer, and if so, is the individual re-contacted if the VUS is reclassified?
This is an important question to ask before testing is performed.
-
What is the cost of testing?
Particularly for individuals who meet criteria for testing, insurance may cover the cost, whereas the consumer is responsible for the costs of consumer-directed testing. However, for individuals who do not meet criteria for testing and/or for whom insurance will not pay, the cost of consumer-directed testing may not be higher than out-of-pocket costs when ordered after pretest genetic counseling.
Some insurance companies require patients to have pretest genetic counseling by a credentialed genetics provider (and to meet specific eligibility criteria) in order for the testing to be covered. Consumer-directed testing thus eliminates the need for this requirement.
Testing for SNPs
In the past, several DTC companies offered only single nucleotide polymorphism (SNP)-based testing to generate information about health risks, including risks of cancer. Selection of SNPs may be based on data from genome-wide association studies (GWAS); however, there is no validated algorithm outlining how to generate cancer risk estimates from different SNPs, which individually are generally associated with modestly increased disease risks (usually conferring odds ratios <2.0) or modestly decreased disease risks.[ 58 ] (Refer to the GWAS section in the Cancer Genetics Overview PDQ summary for more information.) As a result, predicted disease risks from different DTC companies may yield different results. For example, a sample comparison of SNP-based risk prediction from two different companies for four different cancers yielded relative risks of 0.64 to 1.42 (excluding the three Ashkenazi BRCA1/BRCA2 founder pathogenic variants).[ 59 ] In addition, because commercial companies use different panels of SNPs, there is seldom concordance about the predicted risks for common diseases, and such risk estimates have not been prospectively validated.[ 60 ][ 61 ]
Another area of investigation is whether predicted disease risks from SNP testing are consistent with family history–based assessments. Studies using data from one commercial personal genomic testing company revealed that there was generally poor concordance between the SNP and family history risk assessment for common cancers such as breast, prostate, and colon.[ 62 ][ 63 ][ 64 ] Importantly, one of these studies highlighted that the majority of individuals with family histories suggestive of hereditary breast/ovarian cancer or Lynch syndrome received SNP results yielding lifetime cancer risks that were average or below average.[ 62 ]
Studies have begun to examine whether SNP testing could be used together with other established risk factors to assess the likelihood of developing cancer. For example, adding SNP data to validated breast cancer prediction tools such as those included in the National Cancer Institute's Breast Cancer Risk Assessment Tool (based on the Gail model) [ 65 ] may improve the accuracy of risk assessment.[ 66 ][ 67 ] However, this approach is not currently FDA-approved.
These findings underscore that SNP testing has not been validated as an accurate risk assessment tool and does not replace the collection, integration, and interpretation of personal and family history risk factor information by qualified health care professionals.
DTC whole-exome/genome sequencing and interpretation
Increasingly, DTC testing companies offer whole-genome sequencing (WGS) or whole-exome sequencing (WES), including SNP data. (Refer to the Clinical Sequencing section in the Cancer Genetics Overview PDQ summary for a description of WGS and WES.) In addition, consumers who submit their DNA to a DTC lab may have access to their raw sequence data and may consult with other companies, websites, and open-access databases for interpretation.[ 68 ][ 69 ] However, these data must be interpreted with caution. A clinical lab found that 40% of variants reported in DTC raw data were false positives (i.e., low analytic validity because the identified variant was not present).[ 70 ] In addition, several variants that were designated as “increased risk” in the raw data were classified as benign by clinical laboratories and public databases.[ 70 ] Given the potential for misinterpretation, which may lead to unnecessary medical procedures or testing, these findings underscore the importance of clinical confirmation of all potentially medically actionable gene variants identified by DTC testing.
Some factors to consider when determining the accuracy and utility of sequence data for cancer (or other disease) risk assessment include the sequencing depth of the genes of interest, whether large rearrangements or gene deletions would be detected, and whether or how positive results are confirmed (e.g., through Sanger sequencing). For example, if sequencing depth is low or rare variants cannot be detected, then there is a concern about false-negative results. There is also a risk that sequence changes will be erroneously labeled as pathogenic when confirmatory testing or different interpretative approaches would determine that the variant identified is benign (false positive). When WES or WGS is performed, VUS are also likely to be identified,[ 71 ] and DTC companies have varying protocols for classification, which may or may not be consistent with national guidelines (e.g., refer to [ 72 ]). In addition, as evidence evolves and variants are reclassified, consumers need to be aware of the process the DTC lab has, if any, for updating information and re-contacting consumers with revised interpretations.
Considerations
There may be potential benefits associated with DTC testing. DTC marketing and provision of genetic tests may promote patient autonomy.[ 59 ] Individuals may develop an increased awareness of the importance of family history, the relationship between risk and family history, the role of genetics in disease, and a better understanding of the value of genetic counseling.[ 73 ] Although results of SNP-based DTC testing appear to motivate some individuals to seek the advice of their doctor, make lifestyle changes, and pursue screening tests,[ 74 ][ 75 ][ 76 ][ 77 ] short-term modest effects on risk perception after notification of an elevated risk (e.g., for cancer) may not significantly alter lifestyle or cancer screening behaviors.[ 78 ][ 79 ] Further, psychological distress has not been widely reported among consumers who have undergone DTC testing for a variety of conditions.[ 76 ] However, little is known about how individuals respond after learning that they carry pathogenic variants in high-risk genes such as BRCA1/BRCA2 when testing is performed within a DTC context and without traditional forms of pre- and posttest genetic education and counseling.
Given the complexity of genomic testing, several professional organizations have released position statements about DTC genetic testing. For example, in 2010, ASCO published a position statement outlining several considerations related to DTC cancer genomic tests, including those mentioned above.[ 1 ] They endorsed pre- and posttest genetic counseling and informed consent by qualified health care professionals. ASCO’s 2015 position statement on genetic and genomic testing for cancer susceptibility reinforces the importance of provider education given the complexity of genomic testing and interpretation and discusses their recommendations for regulatory review of genomic tests, including those offered by DTC companies.[ 2 ]
In 2016, a statement by the American College of Medical Genetics and Genomics about DTC genetic testing similarly endorsed the involvement of qualified genetics professionals in the processes of test ordering and interpretation.[ 80 ] The statement also emphasized the need to incorporate established methods of risk assessment into disease risk prediction (such as personal and family medical history information) and stressed that consumers need to be informed about the potential limitations and risks associated with DTC testing.
Informed Consent
Informed consent can enhance preparedness for testing, including careful weighing of benefits and limitations of testing, minimization of adverse psychosocial outcomes, appropriate use of medical options, and a strengthened provider-patient relationship based on honesty, support, and trust.
Consensus exists among experts that a process of informed consent should be an integral part of the pretest counseling process.[ 81 ] This view is driven by several ethical dilemmas that can arise in genetic susceptibility testing. The most commonly cited concern is the possibility of insurance or employment discrimination if a test result, or even the fact that an individual has sought or is seeking testing, is disclosed. In 2008, Congress passed the Genetic Information Nondiscrimination Act (GINA). This federal law provides protections related to health insurance and employment discrimination based on genetic information. However, GINA does not cover life, disability, or long-term-care insurance discrimination.[ 82 ] (Refer to the GINA section of this summary for more information.) A related issue involves stigmatization that may occur when an individual who may never develop the condition in question, or may not do so for decades, receives genetic information and is labeled or labels himself or herself as ill. Finally, in the case of genetic testing, medical information given to one individual has immediate implications for biologic relatives. These implications include not only the medical risks but also disruptions in familial relationships. The possibility for coercion exists when one family member wants to be tested but, to do so optimally, must first obtain genetic material or information from other family members.
Inclusion of an informed consent process in counseling can facilitate patient autonomy.[ 83 ] It may also reduce the potential for misunderstanding between patient and provider. Many clinical programs provide opportunities for individuals to review their informed consent during the genetic testing and counseling process. Initial informed consent provides a verbal and/or written overview of the process.
Some programs use a second informed consent process prior to disclosure to the individual of his or her genetic test results. This process allows for the possibility that a person may change his or her mind about receiving test results. After the test result has been disclosed, a third informed consent discussion often occurs. This discussion concerns issues regarding sharing the genetic test result with health providers and/or interested family members, currently or in the future. Obtaining written permission to provide the test result to others in the family who are at risk can avoid vexing problems in the future should the individual not be available to release his or her results.
Core elements of informed consent
Major elements of an informed consent discussion are highlighted in the preceding discussion. The critical elements, as described in the literature,[ 1 ][ 2 ][ 84 ][ 85 ] include the following:
All individuals considering genetic testing should be informed that they have several options even after the genetic testing has been completed. They may decide to receive the results at the posttest meeting, delay result notification, or less commonly, not receive the results of testing. They should be informed that their interest in receiving results will be addressed at the beginning of the posttest meeting and that time will be available to review their concerns and thoughts on notification. It is important that individuals receive this information during the pretest counseling to ensure added comfort with the decision to decline or defer result notification even when test results become available.
Testing in children
Genetic testing for pathogenic variants in cancer susceptibility genes in children is particularly complex. While both parents [ 86 ] and providers [ 87 ] may request or recommend testing for minor children, many experts recommend that unless there is evidence that the test result will influence the medical management of the child or adolescent, genetic testing should be deferred until legal adulthood (age 18 y or older) because of concerns about autonomy, potential discrimination, and possible psychosocial effects.[ 88 ][ 89 ][ 90 ] A number of cancer syndromes include childhood disease risk, such as retinoblastoma, multiple endocrine neoplasia (MEN) types 1 and 2 (MEN1 and MEN2), neurofibromatosis types 1 and 2 (NF1 and NF2), Beckwith–Wiedemann syndrome, Fanconi anemia, FAP, and Von Hippel-Lindau disease (VHL).[ 91 ][ 92 ] As a consequence, decisions about genetic testing in children are made in the context of a specific gene in which a pathogenic variant is suspected. The ASCO statement on genetic testing for cancer susceptibility maintains that the decision to consider offering childhood genetic testing should take into account not only the risk of childhood malignancy but also the evidence associated with risk reduction interventions for that disorder.[ 1 ] Specifically, ASCO recommends that:
Special considerations are required when genetic counseling and testing for pathogenic variants in cancer susceptibility genes are considered in children. The first issue is the age of the child. Young children, especially those younger than 10 years, may not be involved or may have limited involvement in the decision to be tested, and some may not participate in the genetic counseling process. In these cases, the child’s parents or other legal surrogate will be involved in the genetic counseling and will ultimately be responsible for making the decision to proceed with testing.[ 1 ][ 93 ] Counseling under these circumstances incorporates a discussion of how test results will be shared with the child when he or she is older.[ 1 ] Children aged 10 to 17 years may have more involvement in the decision-making process.[ 94 ] In a qualitative study of parents and children aged 10 to 17 years assessing decision making for genetic research participation, older, more mature children and families with open communication styles were more likely to have joint decision making. The majority of children in this study felt that they should have the right to make the final decision for genetic research participation, although many would seek input from their parents.[ 94 ] While this study is specific to genetic research participation, the findings allude to the importance children aged 10 to 17 years place on personal decision making regarding factors that impact them. Unfortunately cognitive and psychosocial development may not consistently correlate with the age of the child.[ 93 ] Therefore, careful assessment of the child’s developmental stage may help in the genetic counseling and testing process to facilitate parent and child adaptation to the test results. Another complicating factor includes potential risks for discrimination. (Refer to the Employment and Insurance Discrimination section in the Ethical, Legal, and Social Implications section of this summary for more information.)
The consequences of genetic testing in children have been reviewed.[ 93 ] In contrast to observations in adults, young children in particular are vulnerable to changes in parent and child bonding based on test results. Genetic testing could interfere with the development of self-concept and self-esteem. Children may also be at risk of developing feelings of survivor guilt or heightened anxiety. All children are especially susceptible to not understanding the testing, results, or implications for their health. As children mature, they begin to have decreased dependency on their parents while developing their personal identity. This can be altered in the setting of a serious health condition or an inherited disorder. Older children are beginning to mature physically and develop intimate relationships while also changing their idealized view of their parents. All of this can be influenced by the results of a genetic test.[ 93 ] In its recommendations for genetic testing in asymptomatic minors, the European Society of Human Genetics emphasizes that parents have a responsibility to inform their children about their genetic risk and to communicate this information in a way that is tailored to the child’s age and developmental level.[ 95 ][ 96 ]
In summary, the decision to proceed with testing in children is based on the use of the test for medical decision making for the child, the ability to interpret the test, and evidence that changes in medical decision making in childhood can positively impact health outcomes. Deferral of genetic testing is suggested when the risk of childhood malignancy is low or absent and/or there is no evidence that interventions can reduce risk.[ 1 ] When offering genetic testing in childhood, consideration of the child’s developmental stage is used to help determine his or her involvement in the testing decision and who has legal authority to provide consent. In addition, careful attention to intrafamilial issues and potential psychosocial consequences of testing in children can enable the provider to deliver support that facilitates adaptation to the test result. (Refer to the PDQ summaries on Genetics of Breast and Gynecologic Cancers; Genetics of Colorectal Cancer; and Genetics of Endocrine and Neuroendocrine Neoplasias for more information about psychosocial research in children being tested for specific cancer susceptibility gene pathogenic variants.)
Testing in vulnerable populations
Genetic counseling and testing requires special considerations when used in vulnerable populations. In 1995, the American Society of Human Genetics published a position statement on the ethical, legal, and psychosocial implications of genetic testing in children and adolescents as a vulnerable population.[ 89 ] However, vulnerable populations encompass more than just children. Federal policy applicable to research involving human subjects, 45 CFR Code of Federal Regulations part 46 Protection Of Human Subjects, considers the following groups as potentially vulnerable populations: prisoners, traumatized and comatose patients, terminally ill patients, elderly/aged persons who are cognitively impaired and/or institutionalized, minorities, students, employees, and individuals from outside the United States. Specific to genetic testing, the International Society of Nurses in Genetics further expanded the definition of vulnerable populations to also include individuals with hearing and language deficits or conditions limiting communication (for example, language differences and concerns with reliable translation), cognitive impairment, psychiatric disturbances, clients undergoing stress due to a family situation, those without financial resources, clients with acute or chronic illness and in end-of-life, and those in whom medication may impair reasoning.
Genetic counseling and testing in vulnerable populations raises special considerations. The aim of genetic counseling is to help people understand and adapt to the medical, psychological, and familial implications of genetic contributions to disease, which in part involves the meaningful exchange of factual information.[ 97 ] In a vulnerable population, health care providers need to be sensitive to factors that can impact the ability of the individual to comprehend the information. In particular, in circumstances of cognitive impairment or intellectual disability, special attention is paid to whether the individual’s legally authorized representative should be involved in the counseling, informed consent, and testing process.
Providers need to assess all patients for their ability to make an uncoerced, autonomous, informed decision prior to proceeding with genetic testing. Populations that do not seem vulnerable (e.g., legally adult college students) may actually be deemed vulnerable because of undue coercion for testing by their parents or the threat of withholding financial support by their parents based on a testing decision inconsistent with the parent’s wishes. Alteration of the genetic counseling and testing process may be necessary depending on the situation, such as counseling and testing in terminally ill individuals who opt for testing for the benefit of their children, but given their impending death, results may have no impact on their own health care or may not be available before their death. In summary, genetic counseling and testing requires that the health care provider assess all individuals for any evidence of vulnerability, and if present, be sensitive to those issues, modify genetic counseling based on the specific circumstances, and avoid causing additional harm.
Importance of Pretest Counseling
The complexity of genetic testing for cancer susceptibility has led experts to suggest that careful, in-depth counseling should precede any decision about the use of testing, in keeping with the accepted principles for the use of genetic testing.[ 98 ]
Qualitative and quantitative research studies indicate that families hold a variety of beliefs about the inheritance of characteristics within families; some of these beliefs are congruent with current scientific understanding, whereas others are not.[ 99 ][ 100 ][ 101 ] These beliefs may be influenced by education, personal and family experiences, and cultural background. Because behavior is likely to be influenced by these beliefs, the usefulness of genetic information may depend on recognizing and addressing the individual’s preexisting cognitions. This process begins with initial discussion and continues throughout the genetic counseling process.
Psychological Impact of Genetic Information/Test Results on the Individual
An accurate assessment of psychosocial functioning and emotional factors related to testing motivation and potential impact and utilization is an important part of pretest counseling.[ 102 ][ 103 ][ 104 ][ 105 ][ 106 ] Generally, a provider inquires about a person’s emotional response to the family history of cancer and also about a person’s response to his or her own risk of developing cancer. People have various coping strategies for dealing with stressful circumstances such as genetic risk. Identifying these strategies and ascertaining how well or poorly they work will have implications for the support necessary during posttest counseling and will help personalize the discussion of anticipated risks and benefits of testing. Taking a brief history of past and current psychiatric symptoms (e.g., depression, extreme anxiety, or suicidality) will allow for an assessment of whether this individual is at particular risk of adverse effects after disclosure of results. In such cases, further psychological assessment may be indicated.
In addition, cognitive deficits in the person being counseled may significantly limit understanding of the genetic information provided and hinder the ability to give informed consent and may also require further psychological assessment. Emotional responses to cancer risk may also affect overall mood and functioning in other areas of life such as home, work, and personal health management, including cancer screening practices.[ 107 ] Education and genetic counseling sessions provide an ongoing opportunity for informal assessment of affective and cognitive aspects of the communication process. Since behavioral factors influence adherence to screening and surveillance recommendations, consideration of emotional barriers is important in helping a person choose prevention strategies and in discussing the potential utility of genetic testing.[ 108 ][ 109 ]
The discussion of issues such as history of depression, anxiety, and suicidal thoughts or tendencies requires sensitivity to the individual. The individual must be assured that the counseling process is a collaborative effort to minimize intrusiveness while maximizing benefits. Determining whether the individual is currently receiving treatment for major psychiatric illness is an important part of the counseling process. Consultation with a mental health professional familiar with psychological assessments may be useful to help the provider develop the strategies for these discussions. It also may be beneficial for the individual to be given standard psychological self-report instruments that assess levels of depression, anxiety, and other psychiatric difficulties that he or she may be experiencing. This step provides objective comparisons with already established normative data.[ 110 ][ 111 ]
In addition to the clinical assessment of psychological functioning, several instruments for cancer patients and people at increased risk of cancer have been utilized to assess psychological status. These include the Center for Epidemiological Studies-Depression scale,[ 112 ] the Profile of Mood States,[ 113 ] the Hospital Anxiety and Depression Scale,[ 114 ] and the Brief Symptom Inventory.[ 115 ] Research programs have included one or more of these instruments as a way of helping refine the selection of people at increased risk of adverse psychosocial consequences of genetic testing. Psychological assessments are an ongoing part of genetic counseling. Some individuals with symptoms of increased distress, extreme avoidance of affect, or other marked psychiatric symptoms may benefit from a discussion with, or evaluation by, a mental health professional. It may be suggested to some people (generally, a very small percentage of any population) that testing be postponed until greater emotional stability has been established.
Psychological Impact of Genetic Information/Test Results on the Family
In addition to making an assessment of the family history of cancer, the family as a social system may also be assessed as part of the process of cancer genetic counseling. Hereditary susceptibility to cancer may affect social interactions and attitudes toward the family.[ 116 ]
In assessing families, characteristics that may be relevant are the organization of the family (including recognition of individuals who propose to speak for or motivate other family members), patterns of communication within the family, cohesion or closeness of family members (or lack thereof), and the family beliefs and values that affect health behaviors. Ethnocultural factors may also play an important role in guiding behavior in some families.
Assessment also evaluates the impact of the family’s prior experience with illness on their attitudes and behaviors related to genetic counseling and testing. Prior experience with cancer diagnosis and treatment, loss due to cancer, and the family members’ interaction with the medical community may heavily influence attitudes toward receiving genetic information and may play a major role in the emotional state of individuals presenting for genetic services.
The practitioner may use the above framework to guide inquiries about the relationship of the individual to (1) the affected members of the family or (2) others who are considering or deciding against the consideration of genetic counseling or testing. Inquiries about how the family shares (or does not share) information about health, illness, and genetic susceptibility may establish whether the individual feels under pressure from other family members or anticipates difficulty in sharing genetic information obtained from counseling or testing. Inquiries about the present health (new diagnoses or deaths from cancer) or relationship status (divorce, marriage, grieving) of family members may inform the provider about the timing of the individual’s participation in counseling or testing and may also reveal possible contraindications for testing at present.
Evidence from a study of 297 persons from 38 Lynch syndrome–affected families suggested that the timing of genetic counseling and testing services may influence psychological test-related distress responses. Specifically, family members in the same generation as the index case were more likely to experience greater test-related distress with increasingly longer lengths of time between the index case's receipt of MMR pathogenic variant results and the provision of genetic counseling and testing services to family members. However, it was unclear whether time lapses were due to a delay in the index case communicating test results or the family member choosing to delay genetic testing, despite being aware of the index case’s results.[ 117 ]
More specific information about family functioning in coping with hereditary cancers can be found in the psychosocial or counseling sections of PDQ summaries on the genetics of specific types of cancer. (Refer to the PDQ summaries on Genetics of Breast and Gynecologic Cancers and Genetics of Colorectal Cancer for more information.)
参考文献- Robson ME, Storm CD, Weitzel J, et al.: American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol 28 (5): 893-901, 2010.[PUBMED Abstract]
- Robson ME, Bradbury AR, Arun B, et al.: American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. J Clin Oncol 33 (31): 3660-7, 2015.[PUBMED Abstract]
- Gustafson SL, Raymond VM, Marvin ML, et al.: Outcomes of genetic evaluation for hereditary cancer syndromes in unaffected individuals. Fam Cancer 14 (1): 167-74, 2015.[PUBMED Abstract]
- Riley BD, Culver JO, Skrzynia C, et al.: Essential elements of genetic cancer risk assessment, counseling, and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns 21 (2): 151-61, 2012.[PUBMED Abstract]
- Clain E, Trosman JR, Douglas MP, et al.: Availability and payer coverage of BRCA1/2 tests and gene panels. Nat Biotechnol 33 (9): 900-2, 2015.[PUBMED Abstract]
- Walcott FL, Dunn BK: Legislation in the genomic era: the Affordable Care Act and genetic testing for cancer risk assessment. Genet Med 17 (12): 962-4, 2015.[PUBMED Abstract]
- The Center for Consumer Information & Insurance Oversight: Affordable Care Act Implementation FAQs - Set 12. Baltimore, Md: Centers for Medicare & Medicaid Services, 2013. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Facing Our Risk of Cancer Empowered (FORCE): Paying for Genetic Services. Tampa, FL: FORCE, 2016. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Offit K, Kohut K, Clagett B, et al.: Cancer genetic testing and assisted reproduction. J Clin Oncol 24 (29): 4775-82, 2006.[PUBMED Abstract]
- Offit K, Sagi M, Hurley K: Preimplantation genetic diagnosis for cancer syndromes: a new challenge for preventive medicine. JAMA 296 (22): 2727-30, 2006.[PUBMED Abstract]
- Wang CW, Hui EC: Ethical, legal and social implications of prenatal and preimplantation genetic testing for cancer susceptibility. Reprod Biomed Online 19 (Suppl 2): 23-33, 2009.[PUBMED Abstract]
- Meyer S, Tischkowitz M, Chandler K, et al.: Fanconi anaemia, BRCA2 mutations and childhood cancer: a developmental perspective from clinical and epidemiological observations with implications for genetic counselling. J Med Genet 51 (2): 71-5, 2014.[PUBMED Abstract]
- Sawyer SL, Tian L, Kähkönen M, et al.: Biallelic mutations in BRCA1 cause a new Fanconi anemia subtype. Cancer Discov 5 (2): 135-42, 2015.[PUBMED Abstract]
- Rich TA, Liu M, Etzel CJ, et al.: Comparison of attitudes regarding preimplantation genetic diagnosis among patients with hereditary cancer syndromes. Fam Cancer 13 (2): 291-9, 2014.[PUBMED Abstract]
- Frank TS, Deffenbaugh AM, Reid JE, et al.: Clinical characteristics of individuals with germline mutations in BRCA1 and BRCA2: analysis of 10,000 individuals. J Clin Oncol 20 (6): 1480-90, 2002.[PUBMED Abstract]
- Nieuwenhuis MH, Vasen HF: Correlations between mutation site in APC and phenotype of familial adenomatous polyposis (FAP): a review of the literature. Crit Rev Oncol Hematol 61 (2): 153-61, 2007.[PUBMED Abstract]
- Knudsen AL, Bülow S, Tomlinson I, et al.: Attenuated familial adenomatous polyposis: results from an international collaborative study. Colorectal Dis 12 (10 Online): e243-9, 2010.[PUBMED Abstract]
- Offit K, Bradbury A, Storm C, et al.: Gene patents and personalized cancer care: impact of the Myriad case on clinical oncology. J Clin Oncol 31 (21): 2743-8, 2013.[PUBMED Abstract]
- Robson M: Multigene panel testing: planning the next generation of research studies in clinical cancer genetics. J Clin Oncol 32 (19): 1987-9, 2014.[PUBMED Abstract]
- Domchek SM, Bradbury A, Garber JE, et al.: Multiplex genetic testing for cancer susceptibility: out on the high wire without a net? J Clin Oncol 31 (10): 1267-70, 2013.[PUBMED Abstract]
- Hiraki S, Rinella ES, Schnabel F, et al.: Cancer risk assessment using genetic panel testing: considerations for clinical application. J Genet Couns 23 (4): 604-17, 2014.[PUBMED Abstract]
- Cragun D, Radford C, Dolinsky JS, et al.: Panel-based testing for inherited colorectal cancer: a descriptive study of clinical testing performed by a US laboratory. Clin Genet 86 (6): 510-20, 2014.[PUBMED Abstract]
- Couch FJ, Hart SN, Sharma P, et al.: Inherited mutations in 17 breast cancer susceptibility genes among a large triple-negative breast cancer cohort unselected for family history of breast cancer. J Clin Oncol 33 (4): 304-11, 2015.[PUBMED Abstract]
- LaDuca H, Stuenkel AJ, Dolinsky JS, et al.: Utilization of multigene panels in hereditary cancer predisposition testing: analysis of more than 2,000 patients. Genet Med 16 (11): 830-7, 2014.[PUBMED Abstract]
- Kurian AW, Hare EE, Mills MA, et al.: Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol 32 (19): 2001-9, 2014.[PUBMED Abstract]
- Tung N, Battelli C, Allen B, et al.: Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer 121 (1): 25-33, 2015.[PUBMED Abstract]
- Moran O, Nikitina D, Royer R, et al.: Revisiting breast cancer patients who previously tested negative for BRCA mutations using a 12-gene panel. Breast Cancer Res Treat 161 (1): 135-142, 2017.[PUBMED Abstract]
- Frey MK, Kim SH, Bassett RY, et al.: Rescreening for genetic mutations using multi-gene panel testing in patients who previously underwent non-informative genetic screening. Gynecol Oncol 139 (2): 211-5, 2015.[PUBMED Abstract]
- Lincoln SE, Kobayashi Y, Anderson MJ, et al.: A Systematic Comparison of Traditional and Multigene Panel Testing for Hereditary Breast and Ovarian Cancer Genes in More Than 1000 Patients. J Mol Diagn 17 (5): 533-44, 2015.[PUBMED Abstract]
- Desmond A, Kurian AW, Gabree M, et al.: Clinical Actionability of Multigene Panel Testing for Hereditary Breast and Ovarian Cancer Risk Assessment. JAMA Oncol 1 (7): 943-51, 2015.[PUBMED Abstract]
- Kapoor NS, Curcio LD, Blakemore CA, et al.: Multigene Panel Testing Detects Equal Rates of Pathogenic BRCA1/2 Mutations and has a Higher Diagnostic Yield Compared to Limited BRCA1/2 Analysis Alone in Patients at Risk for Hereditary Breast Cancer. Ann Surg Oncol 22 (10): 3282-8, 2015.[PUBMED Abstract]
- Ricker C, Culver JO, Lowstuter K, et al.: Increased yield of actionable mutations using multi-gene panels to assess hereditary cancer susceptibility in an ethnically diverse clinical cohort. Cancer Genet 209 (4): 130-7, 2016.[PUBMED Abstract]
- Hermel DJ, McKinnon WC, Wood ME, et al.: Multi-gene panel testing for hereditary cancer susceptibility in a rural Familial Cancer Program. Fam Cancer 16 (1): 159-166, 2017.[PUBMED Abstract]
- Eliade M, Skrzypski J, Baurand A, et al.: The transfer of multigene panel testing for hereditary breast and ovarian cancer to healthcare: What are the implications for the management of patients and families? Oncotarget 8 (2): 1957-1971, 2017.[PUBMED Abstract]
- Yurgelun MB, Allen B, Kaldate RR, et al.: Identification of a Variety of Mutations in Cancer Predisposition Genes in Patients With Suspected Lynch Syndrome. Gastroenterology 149 (3): 604-13.e20, 2015.[PUBMED Abstract]
- Susswein LR, Marshall ML, Nusbaum R, et al.: Pathogenic and likely pathogenic variant prevalence among the first 10,000 patients referred for next-generation cancer panel testing. Genet Med 18 (8): 823-32, 2016.[PUBMED Abstract]
- Shirts BH, Casadei S, Jacobson AL, et al.: Improving performance of multigene panels for genomic analysis of cancer predisposition. Genet Med 18 (10): 974-81, 2016.[PUBMED Abstract]
- Caswell-Jin JL, Gupta T, Hall E, et al.: Racial/ethnic differences in multiple-gene sequencing results for hereditary cancer risk. Genet Med 20 (2): 234-239, 2018.[PUBMED Abstract]
- Rosenthal ET, Bernhisel R, Brown K, et al.: Clinical testing with a panel of 25 genes associated with increased cancer risk results in a significant increase in clinically significant findings across a broad range of cancer histories. Cancer Genet 218-219: 58-68, 2017.[PUBMED Abstract]
- Fecteau H, Vogel KJ, Hanson K, et al.: The evolution of cancer risk assessment in the era of next generation sequencing. J Genet Couns 23 (4): 633-9, 2014.[PUBMED Abstract]
- Hall MJ, Forman AD, Pilarski R, et al.: Gene panel testing for inherited cancer risk. J Natl Compr Canc Netw 12 (9): 1339-46, 2014.[PUBMED Abstract]
- Easton DF, Pharoah PD, Antoniou AC, et al.: Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med 372 (23): 2243-57, 2015.[PUBMED Abstract]
- Eggington JM, Bowles KR, Moyes K, et al.: A comprehensive laboratory-based program for classification of variants of uncertain significance in hereditary cancer genes. Clin Genet 86 (3): 229-37, 2014.[PUBMED Abstract]
- Wolfe Schneider K, Anguiano A, Axell L, et al.: Collaboration of colorado cancer genetic counselors to integrate next generation sequencing panels into clinical practice. J Genet Couns 23 (4): 640-6, 2014.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 1.2020. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed December 23, 2019.[PUBMED Abstract]
- Tung N, Domchek SM, Stadler Z, et al.: Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat Rev Clin Oncol 13 (9): 581-8, 2016.[PUBMED Abstract]
- Hudson KL, Murphy JA, Kaufman DJ, et al.: Oversight of US genetic testing laboratories. Nat Biotechnol 24 (9): 1083-90, 2006.[PUBMED Abstract]
- Schwartz MK: Genetic testing and the clinical laboratory improvement amendments of 1988: present and future. Clin Chem 45 (5): 739-45, 1999.[PUBMED Abstract]
- Javitt GH, Hudson K: Federal neglect: regulation of genetic testing. Issues Sci Technol 22: 58-66, 2006. Also available online. Last accessed February 26, 2020.[PUBMED Abstract]
- McGovern MM, Benach M, Wallenstein S, et al.: Personnel standards and quality assurance practices of biochemical genetic testing laboratories in the United States. Arch Pathol Lab Med 127 (1): 71-6, 2003.[PUBMED Abstract]
- McGovern MM, Elles R, Beretta I, et al.: Report of an international survey of molecular genetic testing laboratories. Community Genet 10 (3): 123-31, 2007.[PUBMED Abstract]
- Ferreira-Gonzalez A, Teutsch S, Williams MS, et al.: US system of oversight for genetic testing: a report from the Secretary's Advisory Committee on Genetics, Health and Society. Per Med 5 (5): 521-528, 2008.[PUBMED Abstract]
- Food and Drug Administration: Notification to Congress: FDA’s Laboratory Developed Tests Framework. Silver Spring, Md: Food and Drug Administration, 2014. Available online. Last accessed May 08, 2020.[PUBMED Abstract]
- U.S. Food and Drug Administration: FDA allows marketing of first direct-to-consumer tests that provide genetic risk information for certain conditions. Silver Spring, Md: U.S. Food and Drug Administration, 2017. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Wanner M: Genomes Versus Exomes Versus Genotypes. Bar Harbor, Me: The Jackson Library, 2016. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- U.S. Food and Drug Administration: FDA authorizes, with special controls, direct-to-consumer test that reports three mutations in the BRCA breast cancer genes. Silver Spring, Md: U.S. Food and Drug Administration, 2018. Available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Ramos E, Weissman SM: The dawn of consumer-directed testing. Am J Med Genet C Semin Med Genet 178 (1): 89-97, 2018.[PUBMED Abstract]
- Couch FJ, Nathanson KL, Offit K: Two decades after BRCA: setting paradigms in personalized cancer care and prevention. Science 343 (6178): 1466-70, 2014.[PUBMED Abstract]
- Bellcross CA, Page PZ, Meaney-Delman D: Direct-to-consumer personal genome testing and cancer risk prediction. Cancer J 18 (4): 293-302, 2012 Jul-Aug.[PUBMED Abstract]
- Swan M: Multigenic condition risk assessment in direct-to-consumer genomic services. Genet Med 12 (5): 279-88, 2010.[PUBMED Abstract]
- Kalf RR, Mihaescu R, Kundu S, et al.: Variations in predicted risks in personal genome testing for common complex diseases. Genet Med 16 (1): 85-91, 2014.[PUBMED Abstract]
- Aiyar L, Shuman C, Hayeems R, et al.: Risk estimates for complex disorders: comparing personal genome testing and family history. Genet Med 16 (3): 231-7, 2014.[PUBMED Abstract]
- Heald B, Edelman E, Eng C: Prospective comparison of family medical history with personal genome screening for risk assessment of common cancers. Eur J Hum Genet 20 (5): 547-51, 2012.[PUBMED Abstract]
- Bloss CS, Topol EJ, Schork NJ: Association of direct-to-consumer genome-wide disease risk estimates and self-reported disease. Genet Epidemiol 36 (1): 66-70, 2012.[PUBMED Abstract]
- Gail MH, Brinton LA, Byar DP, et al.: Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst 81 (24): 1879-86, 1989.[PUBMED Abstract]
- McCarthy AM, Armstrong K, Handorf E, et al.: Incremental impact of breast cancer SNP panel on risk classification in a screening population of white and African American women. Breast Cancer Res Treat 138 (3): 889-98, 2013.[PUBMED Abstract]
- Mealiffe ME, Stokowski RP, Rhees BK, et al.: Assessment of clinical validity of a breast cancer risk model combining genetic and clinical information. J Natl Cancer Inst 102 (21): 1618-27, 2010.[PUBMED Abstract]
- Glusman G, Cariaso M, Jimenez R, et al.: Low budget analysis of Direct-To-Consumer genomic testing familial data. F1000Res 1: 3, 2012.[PUBMED Abstract]
- Cariaso M, Lennon G: SNPedia: a wiki supporting personal genome annotation, interpretation and analysis. Nucleic Acids Res 40 (Database issue): D1308-12, 2012.[PUBMED Abstract]
- Tandy-Connor S, Guiltinan J, Krempely K, et al.: False-positive results released by direct-to-consumer genetic tests highlight the importance of clinical confirmation testing for appropriate patient care. Genet Med 20 (12): 1515-1521, 2018.[PUBMED Abstract]
- Berg JS, Khoury MJ, Evans JP: Deploying whole genome sequencing in clinical practice and public health: meeting the challenge one bin at a time. Genet Med 13 (6): 499-504, 2011.[PUBMED Abstract]
- Richards S, Aziz N, Bale S, et al.: Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 17 (5): 405-24, 2015.[PUBMED Abstract]
- McCabe LL, McCabe ER: Direct-to-consumer genetic testing: access and marketing. Genet Med 6 (1): 58-9, 2004 Jan-Feb.[PUBMED Abstract]
- Bansback N, Sizto S, Guh D, et al.: The effect of direct-to-consumer genetic tests on anticipated affect and health-seeking behaviors: a pilot survey. Genet Test Mol Biomarkers 16 (10): 1165-71, 2012.[PUBMED Abstract]
- Kaufman DJ, Bollinger JM, Dvoskin RL, et al.: Risky business: risk perception and the use of medical services among customers of DTC personal genetic testing. J Genet Couns 21 (3): 413-22, 2012.[PUBMED Abstract]
- Bloss CS, Schork NJ, Topol EJ: Effect of direct-to-consumer genomewide profiling to assess disease risk. N Engl J Med 364 (6): 524-34, 2011.[PUBMED Abstract]
- van der Wouden CH, Carere DA, Maitland-van der Zee AH, et al.: Consumer Perceptions of Interactions With Primary Care Providers After Direct-to-Consumer Personal Genomic Testing. Ann Intern Med 164 (8): 513-22, 2016.[PUBMED Abstract]
- Carere DA, VanderWeele T, Moreno TA, et al.: The impact of direct-to-consumer personal genomic testing on perceived risk of breast, prostate, colorectal, and lung cancer: findings from the PGen study. BMC Med Genomics 8: 63, 2015.[PUBMED Abstract]
- Gray SW, Gollust SE, Carere DA, et al.: Personal Genomic Testing for Cancer Risk: Results From the Impact of Personal Genomics Study. J Clin Oncol 35 (6): 636-644, 2017.[PUBMED Abstract]
- ACMG Board of Directors: Direct-to-consumer genetic testing: a revised position statement of the American College of Medical Genetics and Genomics. Genet Med 18 (2): 207-8, 2016.[PUBMED Abstract]
- Geller G, Botkin JR, Green MJ, et al.: Genetic testing for susceptibility to adult-onset cancer. The process and content of informed consent. JAMA 277 (18): 1467-74, 1997.[PUBMED Abstract]
- Hudson KL, Holohan MK, Collins FS: Keeping pace with the times--the Genetic Information Nondiscrimination Act of 2008. N Engl J Med 358 (25): 2661-3, 2008.[PUBMED Abstract]
- Geller G, Doksum T, Bernhardt BA, et al.: Participation in breast cancer susceptibility testing protocols: influence of recruitment source, altruism, and family involvement on women's decisions. Cancer Epidemiol Biomarkers Prev 8 (4 Pt 2): 377-83, 1999.[PUBMED Abstract]
- American College of Medical Genetics: Genetic susceptibility to breast and ovarian cancer: assessment, counseling and testing guidelines. New York: New York State Department of Health, American College of Medical Genetics Foundation, 1999.[PUBMED Abstract]
- McKinnon WC, Baty BJ, Bennett RL, et al.: Predisposition genetic testing for late-onset disorders in adults. A position paper of the National Society of Genetic Counselors. JAMA 278 (15): 1217-20, 1997.[PUBMED Abstract]
- Bradbury AR, Patrick-Miller L, Egleston B, et al.: Parent opinions regarding the genetic testing of minors for BRCA1/2. J Clin Oncol 28 (21): 3498-505, 2010.[PUBMED Abstract]
- O'Neill SC, Peshkin BN, Luta G, et al.: Primary care providers' willingness to recommend BRCA1/2 testing to adolescents. Fam Cancer 9 (1): 43-50, 2010.[PUBMED Abstract]
- Nelson RM, Botkjin JR, Kodish ED, et al.: Ethical issues with genetic testing in pediatrics. Pediatrics 107 (6): 1451-5, 2001.[PUBMED Abstract]
- Points to consider: ethical, legal, and psychosocial implications of genetic testing in children and adolescents. American Society of Human Genetics Board of Directors, American College of Medical Genetics Board of Directors. Am J Hum Genet 57 (5): 1233-41, 1995.[PUBMED Abstract]
- Wertz DC, Fanos JH, Reilly PR: Genetic testing for children and adolescents. Who decides? JAMA 272 (11): 875-81, 1994.[PUBMED Abstract]
- Field M, Shanley S, Kirk J: Inherited cancer susceptibility syndromes in paediatric practice. J Paediatr Child Health 43 (4): 219-29, 2007.[PUBMED Abstract]
- Tischkowitz M, Rosser E: Inherited cancer in children: practical/ethical problems and challenges. Eur J Cancer 40 (16): 2459-70, 2004.[PUBMED Abstract]
- Fanos JH: Developmental tasks of childhood and adolescence: implications for genetic testing. Am J Med Genet 71 (1): 22-8, 1997.[PUBMED Abstract]
- Bernhardt BA, Tambor ES, Fraser G, et al.: Parents' and children's attitudes toward the enrollment of minors in genetic susceptibility research: implications for informed consent. Am J Med Genet A 116 (4): 315-23, 2003.[PUBMED Abstract]
- European Society of Human Genetics: Genetic testing in asymptomatic minors: Recommendations of the European Society of Human Genetics. Eur J Hum Genet 17 (6): 720-1, 2009.[PUBMED Abstract]
- Borry P, Evers-Kiebooms G, Cornel MC, et al.: Genetic testing in asymptomatic minors: background considerations towards ESHG Recommendations. Eur J Hum Genet 17 (6): 711-9, 2009.[PUBMED Abstract]
- Resta R, Biesecker BB, Bennett RL, et al.: A new definition of Genetic Counseling: National Society of Genetic Counselors' Task Force report. J Genet Couns 15 (2): 77-83, 2006.[PUBMED Abstract]
- National Research Council Committee for the Study of Inborn Errors of Metabolism: Genetic Screening Programs, Principles, and Research. Washington, D.C.: National Academy of Sciences, 1975.[PUBMED Abstract]
- Tessaro I, Borstelmann N, Regan K, et al.: Genetic testing for susceptibility to breast cancer: findings from women's focus groups. J Womens Health 6 (3): 317-27, 1997.[PUBMED Abstract]
- Richards M: Families, kinship and genetics. In: Marteau T, Richards M, eds.: The Troubled Helix: Social and Psychological Implications of the New Human Genetics. Cambridge, England: Cambridge University Press, 1996, pp 249-273.[PUBMED Abstract]
- Hallowell N, Statham H, Murton F: Women's understanding of their risk of developing breast/ovarian cancer before and after genetic counseling. J Genet Couns 7 (4): 345-64, 1998.[PUBMED Abstract]
- Baum A, Friedman AL, Zakowski SG: Stress and genetic testing for disease risk. Health Psychol 16 (1): 8-19, 1997.[PUBMED Abstract]
- Peters JA, Stopfer JE: Role of the genetic counselor in familial cancer. Oncology (Huntingt) 10 (2): 159-66, 175; discussion 176-6, 178, 1996.[PUBMED Abstract]
- Richards M: Families, kinship and genetics. In: Marteau T, Richards M, eds.: The Troubled Helix: Social and Psychological Implications of the New Human Genetics. Cambridge, England: Cambridge University Press, 1996, pp 264-265.[PUBMED Abstract]
- Croyle RT, Achilles JS, Lerman C: Psychologic aspects of cancer genetic testing: a research update for clinicians. Cancer 80 (3 Suppl): 569-75, 1997.[PUBMED Abstract]
- Kessler S: Psychological aspects of genetic counseling, X: advanced counseling techniques. J Genet Couns 6 (4): 379-92, 1997.[PUBMED Abstract]
- van Dooren S, Rijnsburger AJ, Seynaeve C, et al.: Psychological distress and breast self-examination frequency in women at increased risk for hereditary or familial breast cancer. Community Genet 6 (4): 235-41, 2003.[PUBMED Abstract]
- Lerman C, Schwartz MD, Lin TH, et al.: The influence of psychological distress on use of genetic testing for cancer risk. J Consult Clin Psychol 65 (3): 414-20, 1997.[PUBMED Abstract]
- Shoda Y, Mischel W, Miller SM, et al.: Psychological interventions and genetic testing: facilitating informed decisions about BRCA1/2 cancer susceptibility. J Clin Psychol Med Settings 5 (1): 3-17, 1998.[PUBMED Abstract]
- Patenaude AF: Genetic Testing for Cancer: Psychological Approaches for Helping Patients and Families. Washington, DC: American Psychological Association, 2005.[PUBMED Abstract]
- Vadaparampil ST, Miree CA, Wilson C, et al.: Psychosocial and behavioral impact of genetic counseling and testing. Breast Dis 27: 97-108, 2006-2007.[PUBMED Abstract]
- Radloff LS: The CES-D scale: a self-report depression scale for research in the general population. Applied Psychological Measurement 1 (3): 385-401, 1977.[PUBMED Abstract]
- McNair D, Lorr M, Droppelman L, et al.: Profile of Mood States. San Diego, Calif: Educational and Industrial Testing Service, 1971.[PUBMED Abstract]
- Ford S, Lewis S, Fallowfield L: Psychological morbidity in newly referred patients with cancer. J Psychosom Res 39 (2): 193-202, 1995.[PUBMED Abstract]
- Derogatis LR, Melisaratos N: The Brief Symptom Inventory: an introductory report. Psychol Med 13 (3): 595-605, 1983.[PUBMED Abstract]
- Rolland JS: Families, Illness, and Disability: An Integrative Treatment Model. New York, NY: BasicBooks, 1994.[PUBMED Abstract]
- Hadley DW, Ashida S, Jenkins JF, et al.: Generation after generation: exploring the psychological impact of providing genetic services through a cascading approach. Genet Med 12 (12): 808-15, 2010.[PUBMED Abstract]
- Education and Counseling About Risk/Risk Communication
-
Specific clinical programs for risk management may be offered to persons with an increased genetic risk of cancer. These programs may differ from those offered to persons of average risk in several ways: screening may be initiated at an earlier age or involve shorter screening intervals; screening strategies not in routine use, such as screening for ovarian cancer, may be offered; and interventions to reduce cancer risk, such as risk-reducing surgery, may be offered. Current recommendations are summarized in the PDQ summaries addressing the genetics of specific cancers.
The goal of genetic education and counseling is to help individuals understand their personal risk status, their options for cancer risk management, and to explore feelings regarding their personal risk status. Counseling focuses on obtaining and giving information, promoting autonomous decision making, and facilitating informed consent if genetic testing is pursued.
Optimally, education and counseling about cancer risk includes providing the following information:
When a clinically valid genetic test is available, education and counseling for genetic testing typically includes the following:
If a second session is held to disclose and interpret genetic test results, education and counseling focuses on the following:
The process of counseling may require more than one visit to address medical, genetic testing, and psychosocial support issues. Additional case-related preparation time is spent before and after the consultation sessions to obtain and review medical records, complete case documentation, seek information about differential diagnoses, identify appropriate laboratories for genetic tests, find patient support groups, research resources, and communicate with or refer to other specialists.[ 1 ]
Information about inherited risk of cancer is growing rapidly. Many of the issues discussed in a counseling session may need to be revisited as new information emerges. At the end of the counseling process, individuals are typically reminded of the possibility that future research may provide new options and/or new information on risk. Individuals may be advised to check in with the health care provider periodically to determine whether new information is sufficient to merit an additional counseling session. The obligation of health care providers to recontact individuals when new genetic testing or treatment options are available is controversial, and standards have not been established.
Methods of Risk Presentation
The usage of numerical probabilities to communicate risk may overestimate the level of risk certainty, especially when wide confidence intervals exist to the estimates or when the individual may differ in important ways from the sample on which the risk estimate was derived. Also, numbers are often inadequate for expressing gut-level or emotional aspects of risk. Finally, there are wide variations in individuals’ level of understanding of mathematical concepts (i.e., numeracy). For all the above reasons, conveying risk in multiple ways, both numerically and verbally, with discussion of important caveats, may be a useful strategy to increase risk comprehension. The numerical format that facilitates the best understanding is natural frequencies because frequencies include information concerning the denominator, the reference group to which the individual may refer. In general, logarithmic scales are to be avoided.[ 2 ] Additionally, important “contextual” risks may be included with the frequency in order to increase risk comprehension; these may include how the person’s risk compares with those who do not have the risk factor in question and the risks associated with common hazards, such as being in a car accident. Additional suggestions include being consistent in risk formats (do not mix odds and percentages), using the same denominator across risk estimates, avoiding decimal points, including base rate information, and providing more explanation if the risk is less than 1%.
The communication of risk may be numerical, verbal, or visual. Use of multiple strategies may increase comprehension and retention of cancer genetic risk information.[ 2 ] Recently, use of visual risk communication strategies has increased (e.g., histograms, pie charts, and Venn diagrams). Visual depictions of risk may be very useful in avoiding problems with comprehension of numbers, but research that confirms this is lacking.[ 3 ][ 4 ] A study published in 2008 examined the use of two different visual aids to communicate breast cancer risk. Women at an increased risk of breast cancer were randomized to receive feedback via a bar graph alone or a bar graph plus a frequency diagram (i.e., highlighted human figures). Results indicate that overall, there were no differences in improved accuracy of risk perception between the two groups, but among those women who inaccurately perceived very high risk at baseline, the group receiving both visual aids showed greater improvement in accuracy.[ 5 ]
Risk Communication
The purpose of risk counseling is to provide individuals with accurate information about their risk, help them understand and interpret their risk, assist them as they use this information to make important health care decisions, and help them make the best possible adjustment to their situation. A systematic review of 28 studies that evaluated communication interventions showed that risk communication benefits users cognitively by increasing their knowledge and understanding of risk perception and does not negatively influence affect (anxiety, cancer-related worry, and depression). Risk communication does not appear to result in a change in use of screening practices and tests. Users received the most benefit from an approach utilizing risk communication along with genetic counseling.[ 6 ][ 7 ] Perceptions of risk are affected by the manner in which risk information is presented, difficulty understanding probability and heredity,[ 8 ][ 9 ] and other psychological processes on the part of individuals and providers.[ 10 ] Risk may be communicated in many ways (e.g., with numbers, words, or graphics; alone or in relation to other risks; as the probability of having an adverse event; in relative or absolute terms; and through combinations of these methods). The way in which risk information is communicated may affect the individual’s perception of the magnitude of that risk. In general, relative risk estimates (e.g., "You have a threefold increased risk of colorectal cancer") are perceived as less informative than absolute risk (e.g., "You have a 25% risk of colorectal cancer") [ 11 ] or risk information presented as a ratio (e.g., 1 in 4).[ 9 ] A strong preference for having BRCA1/BRCA2 pathogenic variant risk estimates expressed numerically is reported by women considering testing.[ 12 ] Individuals associate widely differing quantitative risks with qualitative descriptors of risk such as “rare” or “common.”[ 13 ] More research is needed on the best methods of communicating risk in order to help individuals develop an accurate understanding of their cancer risks.
Communication Strategies
Recent descriptive examination of the process of cancer genetic counseling has found that counseling sessions are predominantly focused on the biomedical teaching required to inform clients of their choices and to put genetic findings in perspective but that attention to psychosocial issues does not detract from teaching goals and may enhance satisfaction in clients undergoing counseling. For instance, one study of communication patterns in 167 pretest counseling sessions for BRCA1 found the sessions to have a predominantly biomedical and educational focus;[ 14 ] however, this approach was client focused, with the counselor and client contributing equally to the dialogue. These authors note that there was a marked diversity in counselor styles, both between counselors and within different sessions, for each counselor. The finding of a didactic style was corroborated by other researchers who examined observer-rated content checklists and videotape of 51 counseling sessions for breast cancer susceptibility.[ 15 ] Of note, genetic counselors seemed to rely on demographic information and breast cancer history to tailor genetic counseling sessions rather than client’s self-reported expectations or psychosocial factors.[ 16 ] Concurrent provision of psychosocial and scientific information may be important in reducing worry in the context of counseling about cancer genetics topics.[ 17 ] An increasing appreciation of language choices may contribute to enhanced understanding and reduced anxiety levels in the session; for example, it was noted that patients may appreciate synonymic choices for the word “mutation,” such as “altered gene”.[ 18 ] Some authors have published recommendations for cultural tailoring of educational materials for the African-American population, such as a large flip chart, including the use of simple language and pictures, culturally identifiable images (e.g., spiritual symbols and tribal patterns), bright colors, and humor.[ 19 ]
Studies have examined novel channels to communicate genetic cancer risk information, deliver psychosocial support, and standardize the genetic counseling process for individuals at increased risk of cancer.[ 20 ][ 21 ][ 22 ][ 23 ][ 24 ][ 25 ][ 26 ][ 27 ] Much of this literature has attempted to make the genetic counseling session more efficient or to limit the need for the counselor to address basic genetic principles in the session to free up time for the client’s personal and emotional concerns about his or her risk. For example, the receipt of genetic feedback for BRCA1/BRCA2 and mismatch repair gene testing by letter, rather than a face-to-face genetic counseling feedback session, has been investigated.[ 28 ] Other modalities include the development of patient assessments or checklists, CD-ROM programs, and interactive computer programs.
Patient assessments or checklists have been developed to facilitate coverage of important areas in the counseling session. One study assessed patients’ psychosocial needs before a hereditary cancer counseling session to determine the assessment’s effect on the session.[ 29 ] A total of 246 participants from two familial cancer clinics were randomly assigned to either an intervention arm in which the counselor received assessment results or a usual care control arm. Study results demonstrated that psychosocial concerns were discussed more frequently among intervention participants than among controls, without affecting session length. Moreover, cancer worry and psychological distress were significantly lower for intervention versus control participants 4 weeks after the counseling session.
A second study compared a feedback checklist completed by 197 women attending a high-risk breast clinic prior to the counseling session to convey prior genetic knowledge and misconceptions to aid the counselor in tailoring the session for that client.[ 22 ] The use of the feedback checklist led to gains in knowledge from the counseling session but did not reduce genetic counseling time, perhaps because the genetic counselor chose to spend time discussing topics such as psychosocial issues. Use of the checklist did decrease the time spent with the medical oncologist, however. The feedback checklist was compared with a CD-ROM that outlined basic genetic concepts and the benefits and limitations of testing and found that those viewing the CD-ROM spent less time with counselors and were less likely to choose to undergo genetic testing. The CD-ROM did not lead to increased knowledge of genetic concepts, as did use of the checklist.
A prospective study evaluated the effects of a CD-ROM decisional support aid for microsatellite instability (MSI) tumor testing in 239 colorectal cancer patients who met the revised Bethesda criteria but who did not meet the Amsterdam criteria.[ 30 ] The study also tested a theoretical model of factors influencing decisional conflict surrounding decisions to pursue MSI tumor testing. Within the study, half of the sample was randomly assigned to receive a brief description of MSI testing within the clinical encounter, and the other half was provided the CD-ROM decisional support aid in addition to the brief description. The CD-ROM and brief description intervention increased knowledge about MSI testing more than the brief description alone did. As a result, decisional conflict decreased because participants felt more prepared to make a decision about the test and had increased perceived benefits of MSI testing.
Other innovative strategies include educational materials and interactive computer technology. In one study, a 13-page color communication aid using a diverse format for conveying risk, including graphic representations and verbal descriptions, was developed.[ 23 ] The authors evaluated the influence of the communication aid in 27 women at high risk of a BRCA1/BRCA2 pathogenic variant and compared those who had read the aid to a comparison sample of 107 women who received standard genetic counseling. Improvements in genetic knowledge and accuracy of risk perception were documented in those who had read the aid, with no differences in anxiety or depression between groups. Personalized, interactive electronic materials have also been developed to aid in genetic education and counseling.[ 24 ][ 25 ] In one study, an interactive computer education program available prior to the genetic counseling session was compared with genetic counseling alone in women undergoing counseling for BRCA1/BRCA2 testing.[ 25 ] Use of the computer program prior to genetic counseling reduced face-time with the genetic counselor, particularly for those at lower risk of a BRCA1/BRCA2 pathogenic variant. Many of the counselors reported that their client’s use of the computer program allowed them to be more efficient and to reallocate time spent in the sessions to clients’ unique concerns.
Videoconferencing is an innovative strategy to facilitate genetic counseling sessions with clients who cannot travel to specialized clinic settings. In 37 individuals in the United Kingdom, real-time video conferencing was compared with face-to-face counseling sessions; both methods were found to improve knowledge and reduce anxiety levels.[ 26 ] Similarly, teleconferencing sessions, in which the client and genetic specialists were able to talk with each other in real time, were used in rural Maine communities [ 27 ] in the pediatric context to convey genetic information and findings for developmental delays and were found to be comparable to in-person consultations in terms of decision-making confidence and satisfaction with the consultations. An Australian study compared the experiences of 106 women who received hereditary breast and ovarian cancer genetic counseling via videoconferencing with the experiences of 89 women who received counseling face to face. Pre- and 1-month postcounseling assessments revealed no significant differences in knowledge gains, satisfaction, cancer-specific anxiety, generalized anxiety, depression, and perceived empathy of the genetic counselor.[ 31 ]
参考文献- Baker DL, Schuette JL, Uhlmann WR, eds.: A Guide to Genetic Counseling. New York, NY: Wiley-Liss, 1998.[PUBMED Abstract]
- Lipkus IM: Numeric, verbal, and visual formats of conveying health risks: suggested best practices and future recommendations. Med Decis Making 27 (5): 696-713, 2007 Sep-Oct.[PUBMED Abstract]
- Ancker JS, Senathirajah Y, Kukafka R, et al.: Design features of graphs in health risk communication: a systematic review. J Am Med Inform Assoc 13 (6): 608-18, 2006 Nov-Dec.[PUBMED Abstract]
- Schapira MM, Nattinger AB, McHorney CA: Frequency or probability? A qualitative study of risk communication formats used in health care. Med Decis Making 21 (6): 459-67, 2001 Nov-Dec.[PUBMED Abstract]
- Ghosh K, Crawford BJ, Pruthi S, et al.: Frequency format diagram and probability chart for breast cancer risk communication: a prospective, randomized trial. BMC Womens Health 8: 18, 2008.[PUBMED Abstract]
- Edwards A, Gray J, Clarke A, et al.: Interventions to improve risk communication in clinical genetics: systematic review. Patient Educ Couns 71 (1): 4-25, 2008.[PUBMED Abstract]
- Edwards A, Unigwe S, Elwyn G, et al.: Personalised risk communication for informed decision making about entering screening programs. Cochrane Database Syst Rev (1): CD001865, 2003.[PUBMED Abstract]
- Marteau TM, van Duijn M, Ellis I: Effects of genetic screening on perceptions of health: a pilot study. J Med Genet 29 (1): 24-6, 1992.[PUBMED Abstract]
- Hopwood P, Howell A, Lalloo F, et al.: Do women understand the odds? Risk perceptions and recall of risk information in women with a family history of breast cancer. Community Genet 6 (4): 214-23, 2003.[PUBMED Abstract]
- Redelmeier DA, Koehler DJ, Liberman V, et al.: Probability judgement in medicine: discounting unspecified possibilities. Med Decis Making 15 (3): 227-30, 1995 Jul-Sep.[PUBMED Abstract]
- Malenka DJ, Baron JA, Johansen S, et al.: The framing effect of relative and absolute risk. J Gen Intern Med 8 (10): 543-8, 1993.[PUBMED Abstract]
- Winer E, Winer N, Bluman L, et al.: Attitudes and risk perceptions of women with breast cancer considering testing for BRCA1/2. [Abstract] Proceedings of the American Society of Clinical Oncology 16: A1937, 537a, 1997.[PUBMED Abstract]
- Mazur DJ, Hickam DH: Patients' interpretations of probability terms. J Gen Intern Med 6 (3): 237-40, 1991 May-Jun.[PUBMED Abstract]
- Ellington L, Baty BJ, McDonald J, et al.: Exploring genetic counseling communication patterns: the role of teaching and counseling approaches. J Genet Couns 15 (3): 179-89, 2006.[PUBMED Abstract]
- Pieterse AH, van Dulmen S, van Dijk S, et al.: Risk communication in completed series of breast cancer genetic counseling visits. Genet Med 8 (11): 688-96, 2006.[PUBMED Abstract]
- Lobb EA, Butow PN, Meiser B, et al.: Tailoring communication in consultations with women from high risk breast cancer families. Br J Cancer 87 (5): 502-8, 2002.[PUBMED Abstract]
- Appleton S, Watson M, Rush R, et al.: A randomised controlled trial of a psychoeducational intervention for women at increased risk of breast cancer. Br J Cancer 90 (1): 41-7, 2004.[PUBMED Abstract]
- Hodgson J, Hughes E, Lambert C: "SLANG"--Sensitive Language and the New Genetics--an exploratory study. J Genet Couns 14 (6): 415-21, 2005.[PUBMED Abstract]
- Baty BJ, Kinney AY, Ellis SM: Developing culturally sensitive cancer genetics communication aids for African Americans. Am J Med Genet 118A (2): 146-55, 2003.[PUBMED Abstract]
- Green MJ, Peterson SK, Baker MW, et al.: Effect of a computer-based decision aid on knowledge, perceptions, and intentions about genetic testing for breast cancer susceptibility: a randomized controlled trial. JAMA 292 (4): 442-52, 2004.[PUBMED Abstract]
- Fransen M, Meertens R, Schrander-Stumpel C: Communication and risk presentation in genetic counseling. Development of a checklist. Patient Educ Couns 61 (1): 126-33, 2006.[PUBMED Abstract]
- Wang C, Gonzalez R, Milliron KJ, et al.: Genetic counseling for BRCA1/2: a randomized controlled trial of two strategies to facilitate the education and counseling process. Am J Med Genet A 134 (1): 66-73, 2005.[PUBMED Abstract]
- Lobb EA, Butow PN, Moore A, et al.: Development of a communication aid to facilitate risk communication in consultations with unaffected women from high risk breast cancer families: a pilot study. J Genet Couns 15 (5): 393-405, 2006.[PUBMED Abstract]
- Mackay J, Schulz P, Rubinelli S, et al.: Online patient education and risk assessment: project OPERA from Cancerbackup. Putting inherited breast cancer risk information into context using argumentation theory. Patient Educ Couns 67 (3): 261-6, 2007.[PUBMED Abstract]
- Green MJ, Peterson SK, Baker MW, et al.: Use of an educational computer program before genetic counseling for breast cancer susceptibility: effects on duration and content of counseling sessions. Genet Med 7 (4): 221-9, 2005.[PUBMED Abstract]
- Coelho JJ, Arnold A, Nayler J, et al.: An assessment of the efficacy of cancer genetic counselling using real-time videoconferencing technology (telemedicine) compared to face-to-face consultations. Eur J Cancer 41 (15): 2257-61, 2005.[PUBMED Abstract]
- Lea DH, Johnson JL, Ellingwood S, et al.: Telegenetics in Maine: Successful clinical and educational service delivery model developed from a 3-year pilot project. Genet Med 7 (1): 21-7, 2005.[PUBMED Abstract]
- Voorwinden JS, Jaspers JP, ter Beest JG, et al.: The introduction of a choice to learn pre-symptomatic DNA test results for BRCA or Lynch syndrome either face-to-face or by letter. Clin Genet 81 (5): 421-9, 2012.[PUBMED Abstract]
- Eijzenga W, Aaronson NK, Hahn DE, et al.: Effect of routine assessment of specific psychosocial problems on personalized communication, counselors’ awareness, and distress levels in cancer genetic counseling practice: a randomized controlled trial. J Clin Oncol 32 (27): 2998-3004, 2014.[PUBMED Abstract]
- Hall MJ, Manne SL, Winkel G, et al.: Effects of a decision support intervention on decisional conflict associated with microsatellite instability testing. Cancer Epidemiol Biomarkers Prev 20 (2): 249-54, 2011.[PUBMED Abstract]
- Zilliacus EM, Meiser B, Lobb EA, et al.: Are videoconferenced consultations as effective as face-to-face consultations for hereditary breast and ovarian cancer genetic counseling? Genet Med 13 (11): 933-41, 2011.[PUBMED Abstract]
- Cancer Genetics Service Delivery
-
Modalities of Genetic Counseling
Cancer risk assessment counseling is a multistep process that traditionally included an in-person pretest and posttest counseling session. In an effort to overcome access barriers, other modalities have been implemented, including group sessions, telephone counseling, and online genetic counseling using remote videoconferencing, which is often referred to as telegenetics.[ 1 ][ 2 ][ 3 ][ 4 ][ 5 ][ 6 ][ 7 ][ 8 ][ 9 ][ 10 ] Of these other modalities, only telephone counseling has been examined for noninferiority against in-person genetic counseling in a randomized controlled trial.[ 11 ][ 12 ][ 13 ][ 14 ]
Telephone genetic counseling
A systematic review identified 13 published studies that used a randomized controlled trial design to compare pretest and posttest outcomes for in-person genetic counseling with telephone counseling. Knowledge and psychosocial outcomes (e.g., distress) were found to be noninferior, equivalent, or not statistically significant between telephone counseling and in-person counseling. Two studies demonstrated lower testing intention or uptake among participants who received telephone counseling. The majority of studies also found no difference in satisfaction; however, two studies demonstrated higher satisfaction among individuals who received telephone compared with those who received in-person genetic counseling.[ 14 ] (The studies were conducted prior to the adoption of multigene panel testing.)
Another group reported results of a study in which all participants (N = 1,178) received in-person pretest counseling at one of five participating sites. Those participants willing to be randomized had their results disclosed by telephone (n = 401) or in person (n = 418). Notably, 30% of participants in this study had multigene panel testing. In this trial, telephone disclosure was noninferior to in-person results disclosure when comparing primary psychosocial outcomes (e.g., general and state anxiety). In primary analysis, knowledge did not meet the threshold of noninferiority without imputing missing data. Secondary outcomes related to cancer distress, depression, uncertainty, satisfaction with genetic testing, and behavioral intentions for risk management strategies were not statistically significant between groups.[ 15 ]
Video-assisted genetic counseling
Studies have also examined the use of online genetic counseling using remote videoconferencing (telegenetics) as an alternative to in-person genetic counseling and demonstrated increases in patient knowledge, high levels of satisfaction, and minimal negative psychosocial outcomes.[ 16 ][ 17 ][ 18 ][ 19 ]
Genetic Service Delivery Models
Emerging approaches to delivering genetic services have been examined to facilitate greater access to genetic counseling and testing. These approaches have been utilized to streamline the process by which high-risk or affected individuals are identified and referred to genetic services. These service delivery models vary in the processes by which patients receive genetic education, counseling, and testing, with genetic counseling increasingly taking place only after genetic testing has already occurred.
Several factors have contributed to the provision of genetic testing without pretest genetic counseling. These factors include: (1) expansion of genetic testing criteria, resulting in increased demand for genetic testing; (2) more indications for testing at the time of cancer diagnosis, given that the identification of a pathogenic variant may affect treatment options (e.g., poly [ADP-ribose] polymerase [PARP]–inhibitors in BRCA1/BRCA2 positive patients with metastatic human epidermal growth factor receptor 2–negative breast cancer, ovarian cancer, or pancreatic cancer); (3) increasing numbers of patients who undergo tumor genomic testing to guide treatment, which may be followed by confirmatory germline testing; (4) increasing availability of universal testing (e.g., for ovarian cancer patients, Ashkenazi Jewish individuals) and consumer-directed genetic testing. Some indications have resulted in patients being offered genetic testing by their health care providers in a nongenetics environment (e.g., by primary care providers, surgeons, or oncologists), which may then be followed by posttest result interpretation and counseling by the provider or via a genetics specialist.
Embedded genetic services
Studies have examined the impact of embedding a cancer genetic counselor on site in gynecologic oncology clinics in efforts to increase referral to and the use of genetic counseling among affected women.[ 20 ][ 21 ][ 22 ] Improvements were observed in referral rates (up to 85%) and genetic counseling uptake following the incorporation of an on-site genetic counselor. Studies reported reductions in time spent with patients by the genetic counselor,[ 20 ] as well as the duration of time between referral to scheduling and completion of a genetic consultation.[ 21 ][ 22 ]
Triaged or streamlined services using nongenetics providers
Nongenetics providers who receive training in cancer genetics are increasingly being used in triaged models to increase access to cancer genetics services. These providers may be engaged at different time points along the risk assessment, counseling, and testing process. In one example, nurses were trained to provide basic risk assessment and offer BRCA testing to patients in an effort to increase access to genetic service providers in rural settings.[ 23 ] Family histories collected via a paper screener administered in mammography or oncology sites were reviewed and triaged by the genetic counselor on the basis of risk status, and subsequent counseling regarding risk was provided by either the nurse or the genetic counselor. A fourfold increase in the number of patients seen at the site was observed over a 2-year period.
In the context of gynecologic oncology, some methodologies have streamlined processes such that oncology physicians conduct pretest education and counseling, informed consent, genetic testing, and return of negative results, while triaging the return of positive or variants of unknown significance results to genetic counselors.[ 22 ][ 24 ] Patient satisfaction with oncologist-led counseling and testing was reported as high, with more than 99% of patients expressing satisfaction in one study.[ 24 ] However, another study involving nongenetics providers in the delivery of genetics services revealed suboptimal outcomes. A study of a single national health insurer in the United States revealed that 37% of women who obtained BRCA1/BRCA2 genetic testing received genetic counseling from a genetics provider prior to testing.[ 25 ] Patients who did not receive pretest genetic counseling by genetics providers were less likely to meet criteria for testing and had lower levels of knowledge, understanding, and satisfaction related to the genetic testing process.
Universal genetic counseling and testing for affected patients
Universal germline genetic testing is now standard practice for patients with certain cancers, including ovarian, pancreatic, and metastatic prostate cancers.[ 26 ] (Refer to the Clinical Application of Genetic Testing for Inherited Prostate Cancer section in the PDQ summary on Genetics of Prostate Cancer for more information about genetic testing in prostate cancer patients.)
The most longstanding guidelines available for universal testing is in ovarian cancer. National guidelines in the United States [ 26 ][ 27 ][ 28 ] and internationally [ 29 ][ 30 ] recommend offering genetic testing to all women with ovarian cancer. There are two primary reasons for the endorsement of universal testing in this patient population, given that up to 15% of ovarian cancer patients harbor a pathogenic variant in BRCA1 or BRCA2:[ 31 ][ 32 ] (1) to identify patients who may benefit from targeted therapy with a PARP-inhibitor, such as olaparib; and (2) to facilitate the identification of at-risk relatives through the process of cascade testing.[ 26 ][ 27 ][ 33 ]
In response, some practices have implemented quality improvement projects that focus on universal referral and genetic testing for ovarian cancer patients.[ 22 ][ 34 ] At one academic gynecologic oncology practice, this included the implementation of several processes including provider and patient education on the rationale behind universal genetic testing, electronic health records modifications to facilitate communication with patients and recommend genetics referral, point-of-care scheduling for genetic counseling at check out, and updates to tumor board conference documentation to include whether genetic counseling was recommended. Uptake of genetic testing increased from 27% to 82% following implementation of these processes over a 3-year period.[ 34 ]
At another institution, the implementation of universal genetic testing across gynecologic oncology clinics also resulted in genetic testing rates that exceeded 80% over a 3-year period.[ 22 ] Notably, different service delivery models were used across clinics to optimize the ability to overcome site constraints and barriers affecting patient access to genetic counseling and testing. These models included 1) physician-coordinated genetic counseling at locations without a genetic counselor on site (triaged/streamlined model), and 2) integrated genetic counseling within the clinic (embedded model).
Population screening: genetic testing without pretest genetics counseling
Patients may be offered genetic testing with limited or no pretest discussion that includes the provision of written or other materials. Studies have used this approach targeting individuals of Ashkenazi Jewish decent for population-based testing.[ 35 ][ 36 ][ 37 ][ 38 ] (The National Comprehensive Cancer Network recommends testing all Ashkenazi Jewish women in a research context.[ 26 ]) In one study, genetic counseling following testing was offered in-person for carriers and noncarriers of BRCA1/BRCA2 pathogenic variants with a significant family history of cancer; letters detailing test results and general screening recommendations were sent for noncarriers with limited family history.[ 35 ] Uptake of BRCA1/BRCA2 testing was 67%, and satisfaction with the population screening approach was greater than 90% at both 1 week and 6 months posttesting. Compliance with posttest counseling was 100% for carriers and 87% for noncarriers with a suggestive family history. Notably, gender differences in compliance were found among noncarriers (89% for women vs. 78% for men; P = .01).[ 35 ]
Direct-to-consumer (DTC) genetic testing
Refer to the DTC Genetic Tests section of this summary for a description of the types of testing offered directly to the consumer and some considerations involving the use of these tests.
参考文献- Ormond K: Recommendations for telephone counseling. J Genet Couns 9 (1): 63-71, 2000.[PUBMED Abstract]
- Sangha K: Assessment of the effectiveness of genetic counseling by telephone compared to a clinic visit. J Genet Couns 12 (2): 171-84, 2003.[PUBMED Abstract]
- Calzone KA, Prindiville SA, Jourkiv O, et al.: Randomized comparison of group versus individual genetic education and counseling for familial breast and/or ovarian cancer. J Clin Oncol 23 (15): 3455-64, 2005.[PUBMED Abstract]
- Jenkins J, Calzone KA, Dimond E, et al.: Randomized comparison of phone versus in-person BRCA1/2 predisposition genetic test result disclosure counseling. Genet Med 9 (8): 487-95, 2007.[PUBMED Abstract]
- Peshkin BN, Demarco TA, Graves KD, et al.: Telephone genetic counseling for high-risk women undergoing BRCA1 and BRCA2 testing: rationale and development of a randomized controlled trial. Genet Test 12 (1): 37-52, 2008.[PUBMED Abstract]
- Zilliacus EM, Meiser B, Lobb EA, et al.: Women's experience of telehealth cancer genetic counseling. J Genet Couns 19 (5): 463-72, 2010.[PUBMED Abstract]
- Rothwell E, Kohlmann W, Jasperson K, et al.: Patient outcomes associated with group and individual genetic counseling formats. Fam Cancer 11 (1): 97-106, 2012.[PUBMED Abstract]
- Platten U, Rantala J, Lindblom A, et al.: The use of telephone in genetic counseling versus in-person counseling: a randomized study on counselees' outcome. Fam Cancer 11 (3): 371-9, 2012.[PUBMED Abstract]
- Benusiglio PR, Di Maria M, Dorling L, et al.: Hereditary breast and ovarian cancer: successful systematic implementation of a group approach to genetic counselling. Fam Cancer 16 (1): 51-56, 2017.[PUBMED Abstract]
- Fournier DM, Bazzell AF, Dains JE: Comparing Outcomes of Genetic Counseling Options in Breast and Ovarian Cancer: An Integrative Review . Oncol Nurs Forum 45 (1): 96-105, 2018.[PUBMED Abstract]
- Schwartz MD, Valdimarsdottir HB, Peshkin BN, et al.: Randomized noninferiority trial of telephone versus in-person genetic counseling for hereditary breast and ovarian cancer. J Clin Oncol 32 (7): 618-26, 2014.[PUBMED Abstract]
- Kinney AY, Steffen LE, Brumbach BH, et al.: Randomized Noninferiority Trial of Telephone Delivery of BRCA1/2 Genetic Counseling Compared With In-Person Counseling: 1-Year Follow-Up. J Clin Oncol 34 (24): 2914-24, 2016.[PUBMED Abstract]
- Kinney AY, Butler KM, Schwartz MD, et al.: Expanding access to BRCA1/2 genetic counseling with telephone delivery: a cluster randomized trial. J Natl Cancer Inst 106 (12): , 2014.[PUBMED Abstract]
- Athens BA, Caldwell SL, Umstead KL, et al.: A Systematic Review of Randomized Controlled Trials to Assess Outcomes of Genetic Counseling. J Genet Couns 26 (5): 902-933, 2017.[PUBMED Abstract]
- Bradbury AR, Patrick-Miller LJ, Egleston BL, et al.: Randomized Noninferiority Trial of Telephone vs In-Person Disclosure of Germline Cancer Genetic Test Results. J Natl Cancer Inst 110 (9): 985-993, 2018.[PUBMED Abstract]
- Otten E, Birnie E, Ranchor AV, et al.: Telegenetics use in presymptomatic genetic counselling: patient evaluations on satisfaction and quality of care. Eur J Hum Genet 24 (4): 513-20, 2016.[PUBMED Abstract]
- Buchanan AH, Datta SK, Skinner CS, et al.: Randomized Trial of Telegenetics vs. In-Person Cancer Genetic Counseling: Cost, Patient Satisfaction and Attendance. J Genet Couns 24 (6): 961-70, 2015.[PUBMED Abstract]
- Bradbury A, Patrick-Miller L, Harris D, et al.: Utilizing Remote Real-Time Videoconferencing to Expand Access to Cancer Genetic Services in Community Practices: A Multicenter Feasibility Study. J Med Internet Res 18 (2): e23, 2016.[PUBMED Abstract]
- Solomons NM, Lamb AE, Lucas FL, et al.: Examination of the Patient-Focused Impact of Cancer Telegenetics Among a Rural Population: Comparison with Traditional In-Person Services. Telemed J E Health 24 (2): 130-138, 2018.[PUBMED Abstract]
- Kentwell M, Dow E, Antill Y, et al.: Mainstreaming cancer genetics: A model integrating germline BRCA testing into routine ovarian cancer clinics. Gynecol Oncol 145 (1): 130-136, 2017.[PUBMED Abstract]
- Senter L, O'Malley DM, Backes FJ, et al.: Genetic consultation embedded in a gynecologic oncology clinic improves compliance with guideline-based care. Gynecol Oncol 147 (1): 110-114, 2017.[PUBMED Abstract]
- Bednar EM, Oakley HD, Sun CC, et al.: A universal genetic testing initiative for patients with high-grade, non-mucinous epithelial ovarian cancer and the implications for cancer treatment. Gynecol Oncol 146 (2): 399-404, 2017.[PUBMED Abstract]
- Cohen SA, Nixon DM: A collaborative approach to cancer risk assessment services using genetic counselor extenders in a multi-system community hospital. Breast Cancer Res Treat 159 (3): 527-34, 2016.[PUBMED Abstract]
- Colombo N, Huang G, Scambia G, et al.: Evaluation of a Streamlined Oncologist-Led BRCA Mutation Testing and Counseling Model for Patients With Ovarian Cancer. J Clin Oncol 36 (13): 1300-1307, 2018.[PUBMED Abstract]
- Armstrong J, Toscano M, Kotchko N, et al.: Utilization and Outcomes of BRCA Genetic Testing and Counseling in a National Commercially Insured Population: The ABOUT Study. JAMA Oncol 1 (9): 1251-60, 2015.[PUBMED Abstract]
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 1.2020. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2019. Available online with free registration. Last accessed December 23, 2019.[PUBMED Abstract]
- Society of Gynecologic Oncology: SGO Clinical Practice Statement: Genetic Testing for Ovarian Cancer. 2014. Available online. Last accessed May 08, 2020.[PUBMED Abstract]
- Hampel H, Bennett RL, Buchanan A, et al.: A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med 17 (1): 70-87, 2015.[PUBMED Abstract]
- Marth C, Hubalek M, Petru E, et al.: AGO Austria recommendations for genetic testing of patients with ovarian cancer. Wien Klin Wochenschr 127 (15-16): 652-4, 2015.[PUBMED Abstract]
- Vergote I, Banerjee S, Gerdes AM, et al.: Current perspectives on recommendations for BRCA genetic testing in ovarian cancer patients. Eur J Cancer 69: 127-134, 2016.[PUBMED Abstract]
- Zhang S, Royer R, Li S, et al.: Frequencies of BRCA1 and BRCA2 mutations among 1,342 unselected patients with invasive ovarian cancer. Gynecol Oncol 121 (2): 353-7, 2011.[PUBMED Abstract]
- Kurian AW, Ward KC, Howlader N, et al.: Genetic Testing and Results in a Population-Based Cohort of Breast Cancer Patients and Ovarian Cancer Patients. J Clin Oncol 37 (15): 1305-1315, 2019.[PUBMED Abstract]
- McCuaig JM, Stockley TL, Shaw P, et al.: Evolution of genetic assessment for BRCA-associated gynaecologic malignancies: a Canadian multisociety roadmap. J Med Genet 55 (9): 571-577, 2018.[PUBMED Abstract]
- Uyar D, Neary J, Monroe A, et al.: Implementation of a quality improvement project for universal genetic testing in women with ovarian cancer. Gynecol Oncol 149 (3): 565-569, 2018.[PUBMED Abstract]
- Lieberman S, Tomer A, Ben-Chetrit A, et al.: Population screening for BRCA1/BRCA2 founder mutations in Ashkenazi Jews: proactive recruitment compared with self-referral. Genet Med 19 (7): 754-762, 2017.[PUBMED Abstract]
- Metcalfe KA, Poll A, Royer R, et al.: Screening for founder mutations in BRCA1 and BRCA2 in unselected Jewish women. J Clin Oncol 28 (3): 387-91, 2010.[PUBMED Abstract]
- Metcalfe KA, Mian N, Enmore M, et al.: Long-term follow-up of Jewish women with a BRCA1 and BRCA2 mutation who underwent population genetic screening. Breast Cancer Res Treat 133 (2): 735-40, 2012.[PUBMED Abstract]
- Gronwald J, Huzarski T, Byrski T, et al.: Direct-to-patient BRCA1 testing: the Twoj Styl experience. Breast Cancer Res Treat 100 (3): 239-45, 2006.[PUBMED Abstract]
- Ethical, Legal, and Social Implications
-
Having an understanding of the ethical, legal, and social implications (ELSI) regarding cancer genetic testing may influence the clinician’s response to the complex questions and issues that may arise during the process of risk assessment and counseling. This section discusses biomedical ethics codes, legal and social issues relevant to privacy, and fair use in the interpretation of genetic information. In order to integrate the different perspectives of bioethics, law, and psychosocial influences, case scenarios are offered to illustrate dilemmas encountered in the clinical setting. (Refer to the Determining the Test to Be Used section of this summary for more information about the regulation of genetic tests.)
Bioethical Issues in Cancer Genetic Testing
Bioethical tenets can guide health care providers in dealing with the complex issues surrounding predictive testing for hereditary cancer. The tenets of beneficence, nonmaleficence, autonomy, and justice are part of a framework needed to balance the complex and potentially conflicting factors surrounding a clinician’s role in respecting privacy, confidentiality and fair use of genetic information obtained from cancer genetic testing.
Beneficence
The concept of beneficence dictates that the primary goal of medical care is to provide benefit through appropriate health care.[ 1 ] In the field of oncology, this translates into using early detection and effective treatment protocols to improve outcomes. Providing beneficent care may go beyond medical outcomes of treatment to encompass the patient’s life circumstances, expectations, and values.[ 1 ] Consideration of the patient’s psychological and emotional ability to handle the testing and results disclosure process can help avoid doing harm.[ 2 ] (Refer to the Psychological Impact of Genetic Testing/Test Results on the Individual section of this summary for more information.)
Nonmaleficence
Nonmaleficence is the bioethical code that directs health care providers to do no harm, inclusive of physical and emotional harm, and acknowledges that medical care involves risks and benefits.[ 1 ] Particular to the field of oncology, adherence to this construct includes taking measures to minimize the adverse effects of cancer prevention, treatment, and control. This may encompass taking precautionary measures to prevent inadvertent disclosure of sensitive information.[ 2 ]
Autonomy
Autonomous decision making respects individual preferences by incorporating informed consent and education.[ 1 ] Individuals have the right to be informed about the risks and benefits of genetic testing and to freely choose or decline testing for themselves. Additionally, it is beneficial to consider the sociocultural context and family dynamics to ensure medical decision making takes places without coercion or interference.[ 1 ]
Justice
Justice refers to the equitable distribution of the benefits and risks of health care.[ 1 ] A goal in oncology is ensuring access to cancer genetic services. The availability of predictive genetic testing should not be dependent on ethnic background, geographical location, or ability to pay. Genetic discrimination should not be a result of predictive testing.[ 2 ] Equitable distribution balances individual rights with responsibilities of community membership.[ 1 ]
Privacy and Confidentiality: Disclosure of Patient’s Genetic Information
A strong provider-patient relationship is founded on respect for the patient’s privacy and confidentiality; therefore, protecting the patient’s personal information from third parties is key to building trust.[ 2 ][ 3 ] Predictive testing for cancer susceptibility presents a challenge because of the hereditary nature of the diseases being tested and the implications of genetic risk for family members. Physicians are faced with a duty to warn or to act to prevent foreseeable harm.[ 4 ] One practical suggestion for facilitating family-based communication is providing patients with education and information materials to facilitate disease susceptibility discussions with family members.[ 1 ] The next section discusses the legal, legislative, and ethical basis for balancing patient confidentiality with duty to warn.
Disclosure in research
Privacy and confidentiality also applies to research, such as population screening for genetic diseases. The U.S. Department of Health and Human Services authorizes the use of Certificates of Confidentiality to researchers.[ 5 ] This certificate, issued by the National Institutes of Health, protects the researcher from having to reveal the identity of any research subject “in any Federal, State, or local civil, criminal, administrative, legislative, or other proceedings.” The protections offered by the certificate of confidentiality are limited to personally identifiable information collected beginning on the date of issuance and ending on the expiration date, which matches the date of study completion. The NIH Office of Extramural Research policy and guidance on Certificates of Confidentiality notes that any personally identifiable information collected during that time interval is protected in perpetuity. In regard to family-based recruitment strategies, the Cancer Genetics Network Bioethics Committee assembled a group of experts to develop recommendations for researchers to use in approaching family members.[ 6 ] Due to the wide spectrum of research strategies, there are different levels of concern. Essential to family-based recruitment strategies is informing potential research participants how their personal information was obtained by the researcher, why the researcher is approaching them, what the researcher knows about them, and for what purpose the information will be used, whether or not they decide to participate.[ 6 ]
“Duty to warn”: Legal proceedings, federal/state legislation, and recommendations of professional organizations
“Duty to warn” requires balancing the bioethical constructs of beneficence and autonomy with other factors such as case proceedings, legislation, and professional societies’ recommendations. As of September 2008, the National Council of State Legislatures lists the states that have legislation requiring consent to disclose genetic information. The definition of "genetic information" can vary depending on the legal case and the language used in state and federal legislation, and generally includes genetic testing and family history information; however, the definition generally does not apply to current diagnoses. Genetic diagnosis can be done through direct genetic tests for disorders linked to a specific gene and indirect genetic tests for disorders in which the specific genes are not known or there are multiple different genes involved (genetic heterogeneity).[ 7 ] There are four state case laws that apply to duty to warn.[ 8 ] Two cases deal directly with testing for hereditary cancer predisposition syndromes; one case deals with a psychotherapist's duty to warn a relative of imminent threat, and another with genetic testing as a tool for reproductive decisions. Table 3 summarizes the cases.
Table 3. State Case Laws That Apply to Duty to Warn State Case Law Description Summary Tarasoff versus Regents of the University of California [ 9 ][ 10 ] Establishes moral duty to warn family members of risks unknown to them In 1976, the California court judged that breach of confidentiality would have been justified in order to warn of a foreseeable and serious harm to an identifiable individual. Distinct from genetic risk since the pathogenic variant is already present (or absent) in family members Pate versus Threlkel [ 8 ][ 11 ][ 12 ] Duty to warn family members of hereditary risk of cancer is satisfied by telling the patient to tell his or her family In 1995, the Florida court judged that a physician had a duty to warn the patient that her children were at risk of developing thyroid cancer because the disease could have been detected and cured at an earlier stage. Safer versus Estate of Pack [ 8 ][ 13 ] Physician must take reasonable steps to warn family members of hereditary risk disease In 1996, a New Jersey appellate court defined a physician’s duty to warn immediate family members of risk of colon cancer; however, the court ruled in favor of the doctor because the patient had undergone rectal screening as a child, which indicated that she had been warned of the risk. Molloy versus Meier [ 8 ][ 14 ] Physician’s duty regarding genetic testing and diagnosis of foreseeable disease risk extends beyond the patient to biological parents In 2004, a Minnesota Supreme Court held that the physician failed to breach confidentiality to warn of hereditary disease risk because he did not inform parents of the diagnosis of fragile X syndrome in their first child. The parents state that this information would have influenced their reproductive decisions. At the federal level, there are strict nondisclosure policies governing private health information.[ 8 ] The Standards for Privacy of Individually Identifiable Health Information (Privacy Rule), which summarizes the Health Insurance Portability and Accountability Act (HIPAA) of 1996, finds it permissible to disclose health information without consent when the public interest is at risk;[ 15 ][ 16 ] therefore, under certain conditions, there are exceptions to the nondisclosure policy include the following:
- There is serious or imminent threat to the health or safety of a person or the public.
- The threat constitutes an imminent, serious threat to an identifiable third party.
- The physician has the capacity to avert significant harm.
Professional societies and government advisory agencies have published their different positions and recommendations on communication between a physician and a patient's relatives in regard to disclosure of genetic disease.[ 4 ][ 8 ][ 17 ]
The Council on Ethical and Judicial Affairs of the American Medical Association (AMA) and the American Society of Clinical Oncology (ASCO) [ 18 ][ 19 ] encourage discussing the importance of patients sharing genetic information with family members.[ 4 ] Specifically, the Council on Ethical and Judicial Affairs of the American Medical Association states that “Physicians …should identify circumstances under which they would expect patients to notify biological relatives of the availability of information related to risk of disease…(and) physicians should make themselves available to assist patients in communicating with relatives to discuss opportunities for counseling and testing, as appropriate.” ASCO’s position is that providers “should remind patients of the importance of communicating test results to family members… ASCO believes that the cancer care provider’s obligations (if any) to at-risk relatives are best fulfilled by communication of familial risk to the person undergoing testing, emphasizing the importance of sharing this information with family members so that they may also benefit.”[ 18 ] These organizations recommend that family members disclose genetic information.
The National Society of Genetic Counselors [ 20 ] and the International Society of Nurses in Genetics [ 21 ] support the release of any genetic information upon request to third parties including relatives but only with the patient's consent.[ 4 ] One of the tenets of genetic counseling is to maintain information received from clients as confidential, unless released by the client or consent for disclosure is provided as required by law.[ 4 ][ 20 ]
Similar to the Privacy Rule, the U.S. Bioethics Commission,[ 22 ] American Society of Human Genetics,[ 23 ] and National Human Genome Research Institute (NHGRI) recommend the following guidelines to identify exceptional circumstances under which it is ethically acceptable to breach confidentiality.[ 4 ][ 8 ]
- There is a high likelihood of harm if the relative is not warned.[ 4 ][ 22 ][ 23 ]
- The patient, despite encouragement, refuses to inform family members.[ 4 ][ 22 ][ 23 ]
- The relative is identifiable.[ 23 ]
- The harm of nondisclosure is greater than the harm of disclosure.[ 23 ]
- Current medical technology renders the disease preventable, treatable, or manageable.[ 23 ]
- Only the information necessary to prevent harm is released.[ 4 ][ 24 ]
- There is no other reasonable way to avert harm.[ 4 ]
At an international level, the World Health Organization and World Medical Association have similar guidelines.[ 4 ] Additionally, Australia, Canada, Germany, Japan, the Netherlands, and the United Kingdom have guidelines supporting the disclosure of genetic information to relatives under similar exceptional circumstances.[ 4 ]
Employment and Insurance Discrimination
Genetic information obtained from genetic susceptibility tests may have medical, economic, and psychosocial implications for the individual tested and his or her family members. The potential for employment and insurance discrimination is a common concern for individuals considering genetic testing.[ 25 ][ 26 ] However, there is limited documentation of the occurrence of employment and insurance discrimination on the basis of hereditary cancer genetic testing results.
(Refer to the Informed Consent subsection of this summary for more information.)
Legal proceedings, federal/state legislation, and recommendations of professional organizations
State and federal legislation statutes have been developed to prevent the use of genetic information for employment practices, such as hiring, promotion, and salary decisions; and insurance policies, including life and health coverage, by employers, schools, government agencies, and insurers.[ 12 ] According to Executive Order 13145, federal departments and agencies are prohibited from discriminating against employees on the basis of genetic test results or information about a request for genetic testing services.[ 24 ] Employers and insurers are prohibited from intentionally lowering policy rates by using practices such as screening for individuals who are at risk of becoming ill or dying due to genetic disease susceptibility, such as cancer.[ 24 ] These provisions were extended by the Genetic Information Nondiscrimination Act (GINA) in 2008. (Refer to the GINA section of this summary for more information.) Federal laws, including GINA, do not cover employer-provided life and disability; however, some states do have legislation addressing the use of genetic information for life and disability policies. The National Conference of State Legislatures (NCSL) [ 27 ][ 28 ] summarized current health legislation of the U.S. Congress. Examples of relevant legislation are summarized in Table 4.
Table 4. Comparison of Federal Legislation Addressing Genetic Coverage, Limitations, and Protectionsa Law Coverage Limitations Protect All Americans aAdapted from Leib et al.[ 29 ] Civil Rights Act of 1964 Employment only Does not apply to health insurance Yes Applies in instances of discrimination based on genetic information if associated with race or ethnic groups Strong association with a racial or ethnic group for hereditary cancers is rare Americans with Disabilities Act of 1990 Disabilities associated with manifesting genetic information Does not apply to health insurance Yes Health Insurance Portability and Accountability Act of 1996 Group health insurance plans Does not stop insurers from requiring genetic tests Yes Genetic information is not defined Forbids excluding an individual in a group health plan due to genetic information Genetic information can be used for plan underwriting Forbids premium increases for different group plan members Disclosure of genetic information is not restricted Preexisting conditions can not include predictive genetic information Does not apply to individual health plans, unless covered by the portability provision Executive Order 13145 of 2000 Forbids Federal employee workplace genetic discrimination Does not apply to health insurance No; excludes members of the United States military and anyone who is NOT a federal employee Only applies to Federal employees Genetic Information Nondiscrimination Act of 2008 (GINA) (Enacted in 2009) Forbids genetic discrimination in the workplace and in health insurance Civil suit is restricted to only those who have had all administrative remedies exhausted No; excludes members of the United States military, veterans obtaining health care through the Veteran’s Administration, and the Indian Health Service Genetic information broadly defined Specific to group and individual insurance plans Forbids use of genetic information in underwriting Forbids requiring genetic testing by employers and insurers Does not cover life, disability, and long-term care insurance Genetic Information Nondiscrimination Act 2008
GINA 2008 protects the provision of health insurance and employment against discrimination based on genetic information as follows:
GINA amends and/or extends coverage of HIPAA, Americans with Disabilities Act (ADA), and Employee Retirement Income Security Act (ERISA) by including genetic information under medical privacy and confidentiality legislation and employment and insurance determinations.[ 27 ] Additionally, with the passage of GINA, researchers and clinicians can encourage participation in clinical trials and appropriate genetic testing knowing that there are federal protections against discrimination based on the results of genetic testing. GINA established the minimum protection level that must be met in all states. However, for states with more robust legislation in place, GINA does not weaken existing protections provided by state law.
However, GINA has several limitations.
- GINA does not apply to members of the United States military, to veterans obtaining health care through the Veteran’s Administration, or to the Indian Health Service because the laws amended by GINA do not apply to these groups and programs.
- The legislation does not apply to life insurance, long-term care insurance, or disability insurance. Even though GINA does not provide protection for employer-provided disability and life insurance, some states do encompass these arenas in addition to employment, genetic privacy, health insurance, health insurance enforcement, life, disability, and long-term care. NHGRI's Genome Statute and Legislation Database provides a searchable listing of state statutes and bills related to the following topics: direct-to-consumer genetic testing, employment and insurance nondiscrimination, health insurance coverage, privacy, research, and the use of residual newborn screening specimens.
- GINA’s employment provisions generally do not apply to employers with fewer than 15 employees.[ 31 ]
Public awareness of GINA and its protections is limited with several studies noting a low level of awareness of the protections that are afforded under this legislation.[ 34 ][ 35 ][ 36 ] Although genetic testing has increased since the passage of the law, relatively few cases of discrimination in which GINA’s authority can be tested have been reported.[ 35 ]
Exception to protections against employment and insurance discrimination: Active duty military personnel
GINA and other state and federal protections do not extend to genetic testing of active duty military personnel or genetic information obtained from active duty military personnel.[ 37 ] In the military, genetic testing provides medical information that is to be used to protect military personnel from harmful duty or other exposures that could stimulate or aggravate a health problem. For example, use of certain antimalaria medication in individuals with glucose 6-phosphate dehydrogenase deficiency can result in red blood cell rupture. Therefore, some genetic information is critical for maintaining the health and safety of military personnel, given the possible stressful occupational environments they face. In addition, all military personnel provide a DNA sample to be maintained in a repository that can be used for identification purposes.[ 38 ]
Results of genetic tests for disease predisposition could influence military eligibility for new enlistments, and for current military personnel, genetic test results could influence worldwide eligibility, assignments, and promotions. For example, a young woman found to carry a BRCA pathogenic variant may not be considered eligible for deployment for 12-15 months because access to recommended health care may not be easily accessible, such as breast MRI, a recommended screening modality for carriers of BRCA pathogenic variants. Active duty military personnel with less than eight years of active duty service are especially vulnerable in the event they become disabled and must go before the medical board to establish benefit eligibility.
In 2006, Department of Defense Instruction Number 1332.38 (DODINST 1332.38) redefined preexisting condition as a result of two cases brought by service members who each had a hereditary condition that presented later in their military careers. The disability instructions state that any injury or disease discovered after a service member enters active duty—with the exception of congenital and hereditary conditions—is presumed to have been incurred in the line of duty. Any hereditary and/or genetic disease shall be presumed to have been incurred prior to entry into active duty. However, DODINST 1332.38 further states that any aggravation of that disease, incurred in the line of duty, beyond that determined to be due to natural progression, shall be deemed service aggravated. As a result of these two cases, the 8-year active duty service limit was established. This means that after 8 or more years of military service, the natural progression of a genetic condition would be deemed aggravated by military service. Therefore, until late 2008, the presence of a congenital or hereditary condition would not be considered a preexisting condition in disability decision making for those with 8 or more years of service.
In October 2008, in response to the National Defense Authorization Act of 2008 (NDAA) Title XVI: “Wounded Warrior Matters,” a policy memorandum was issued providing supplemental and clarifying guidance on implementing disability-related provisions, including new language related to hereditary or genetic diseases. The policy memorandum states, “Any hereditary or genetic disease shall be evaluated to determine whether clear and unmistakable evidence demonstrates that the disability existed before the Service member’s entrance on active duty and was not aggravated by military service. However, even if the conclusion is that the disability was incurred prior to entry on active duty, any aggravation of that disease, incurred while the member is entitled to basic pay, beyond that determined to be due to natural progression shall be determined to be service aggravated.” The interpretation of this policy is uncertain at this time.[ 38 ]
Case scenarios involving ELSI issues in cancer genetic testing
There are multiple psychosocial, ethical, and legal issues to consider in cancer genetic testing. Genetic tests for germline pathogenic variants have social and family implications. In addition to prevention and surveillance options, genetic testing should be offered in conjunction with genetic education and counseling.[ 18 ][ 19 ] A comprehensive strategy for dealing with ethical dilemmas can incorporate a shared approach to decision making, including open discussion, planning, and involvement of the family.[ 5 ] To integrate the different perspectives of bioethics, law, and psychosocial influences, the following scenarios can help health care providers become familiar with commonly encountered dilemmas; it is imperative, however, that the clinician evaluate each patient and his or her situation on a case-by-case basis. These case scenarios were adopted from “Counseling about Cancer: Strategies for Genetic Counseling;” the in-depth case examples are extensively discussed in the original text.[ 2 ]
Duty to warn versus privacy
A patient with known family history of breast cancer is interested in testing for BRCA1 and BRCA2 pathogenic variant. In reviewing her family history, the health care provider realizes that the patient is not aware of an additional rare but hereditary cancer pathogenic variant in a second-degree relative, which the health center tested and confirmed in the past. After talking with her family, the patient is unable to confirm the details of the second hereditary cancer pathogenic variant and again expresses interest in BRCA1/BRCA2 testing. Does the health care provider have a “duty to warn” the patient of the unknown cancer susceptibility gene in the family, at the risk of disclosing private patient information? The following issues are important to consider in resolving this case.
- Preserving the confidentiality of the relative and informing the patient of her cancer risk are both important goals. In general, the health care professional has a “Duty to warn” when there is a high likelihood of harm if not warned, the person at risk is identifiable, the harm of nondisclosure is greater than disclosure, and only the information necessary to prevent harm is released. (Refer to the Privacy and Confidentiality: Disclosure of Patient’s Genetic Information section of this summary for more information.)
- It is possible that the benefit outweighs the harm of informing the patient of the second cancer syndrome because the monitoring and management of the rare cancer are different from guidelines for the general population. Additionally both parties are identifiable. An option is to contact the relative for permission to disclose the genetic test result to the patient in question.
- If it is not possible to obtain permission to disclose, it is possible to inform the patient that she meets clinical criteria for the hereditary cancer syndrome without releasing specific information about the genetic test results of the relative.
Patient’s right to know versus family member’s autonomy
A patient with a family history of a hereditary cancer is interested in predictive genetic testing and convinces an affected family member, who initially expresses unwillingness, to be tested in order to establish the familial pathogenic variant. In this scenario, the surviving family member admits to feeling pressured into consenting for genetic testing. Both the patient and the affected family member are patients. What takes precedence—the patient’s right to know or the family member’s autonomy? The following issues are important to consider in resolving this case.
- Explore, with the patient, alternatives to testing that do not involve the participation of the unwilling family member, such as testing stored tissue of a deceased relative. (Refer to the Value of testing an affected family member first section of this summary for more information).
- If the patient does not want to consider other options and the family member has agreed to be tested without coercion or interference, inform the family member of the implications of the test results, including risks and benefits, and assess her emotional well-being prior to testing.[ 20 ] (Refer to the Informed Consent section of this summary for more information.)
Right to know versus right not to know
A hereditary cancer syndrome has been identified in a family. Within that family, an adult child wants a cancer susceptibility test that her parent declined, and one identical twin wants testing but the other does not. Even though the uninterested parties have declined testing and do not want to know the results, it is possible that testing one relative can disclose results for the other family members. Do the rights of the family members interested in predictive testing take precedence over the rights of the relatives who do not want to know? The following issues are important to consider in resolving this case.
- In hereditary cancer syndromes, an individual’s right to know takes precedence over an individual’s right not to know especially if there are early detection and prevention strategies to reduce the likelihood of morbidity and mortality.
- Since the family has a documented pathogenic variant, standard of care recommendations include guidelines for screening and monitoring. In the event that testing is not done, it is important to take “reasonable steps” to guarantee immediate family members are warned of the hereditary cancer risk. (Refer to the Privacy and Confidentiality: Disclosure of Patient’s Genetic Information section of this summary for more information.)
- Pretest and posttest discussions can include the possibility of medical, psychological, and social impact on family members and strategies on how to lessen any negative impact. The patient should honor the wishes of relatives who request not to know and attempt to keep the results secret.[ 20 ]
Beneficence versus paternalism
A psychological assessment of a patient interested in predictive testing for an autosomal dominant cancer reveals a history of depression and suicidal attempts. The health care provider is considering denying or deferring testing because of concerns for the patient’s emotional well-being even though the patient refuses a referral to a psychologist because he reports feeling emotionally stable. Is deferring or denying predictive genetic testing a beneficent gesture or an act of paternalism? The following issues are important to consider in resolving this case.
- Despite the patient’s refusal to speak with a psychologist, the health care provider can discuss the details of the case with a mental health professional to determine suicidal risk. (Refer to the Psychological Impact of Genetic Information/Test Results on the Individual section of this summary for more information.)
- If there is risk of psychosocial disturbances because of test results, it is possible to defer testing. Conditions under which testing can resume are explained to the patient. For example, the NSGC Code of Ethics recommends that clients be referred to other qualified professionals when the patient requires additional services.[ 20 ]
- Denying a test does not seem justifiable under any circumstances because it implies that the client will never be able to undergo testing.
Professional guidelines and other resources
(Refer to the Genetic Resources section of the PDQ Cancer Genetics Overview summary for more information about the ELSI of genetic testing and counseling.)
参考文献- Burke W, Press N: Genetics as a tool to improve cancer outcomes: ethics and policy. Nat Rev Cancer 6 (6): 476-82, 2006.[PUBMED Abstract]
- Schneider K: The ethical issues. In: Schneider KA: Counseling About Cancer: Strategies for Genetic Counseling. 2nd ed. New York, NY: Wiley-Liss, 2002, pp 291-312.[PUBMED Abstract]
- Offit K: Clinical Cancer Genetics: Risk Counseling and Management. New York, NY: John Wiley and Sons, 1998.[PUBMED Abstract]
- Godard B, Hurlimann T, Letendre M, et al.: Guidelines for disclosing genetic information to family members: from development to use. Fam Cancer 5 (1): 103-16, 2006.[PUBMED Abstract]
- Offit K: Psychological, ethical, and legal issues in cancer risk counseling. In: Offit K: Clinical Cancer Genetics: Risk Counseling and Management. New York, NY: John Wiley and Sons, 1998, pp 287-315.[PUBMED Abstract]
- Beskow LM, Botkin JR, Daly M, et al.: Ethical issues in identifying and recruiting participants for familial genetic research. Am J Med Genet A 130A (4): 424-31, 2004.[PUBMED Abstract]
- Tantravahi U, Wheeler P: Molecular genetic testing for prenatal diagnosis. Clin Lab Med 23 (2): 481-502, 2003.[PUBMED Abstract]
- Offit K, Groeger E, Turner S, et al.: The "duty to warn" a patient's family members about hereditary disease risks. JAMA 292 (12): 1469-73, 2004.[PUBMED Abstract]
- California requires psychiatrists to warn about dangerous patients - Tarasoff v. Regents of University of California, 17 Cal. 3d 425, 551 P.2d 334, 131 Cal. Rptr. 14 (Cal. 1976). 1976. Also available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Harris M, Winship I, Spriggs M: Controversies and ethical issues in cancer-genetics clinics. Lancet Oncol 6 (5): 301-10, 2005.[PUBMED Abstract]
- Pate v. Threlkel, 661 So. 2d 278 (Florida 1995). 1995. Also available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Sankar P: Genetic privacy. Annu Rev Med 54: 393-407, 2003.[PUBMED Abstract]
- Safer v. Estate of Pack, 677 A2d 1188 (NJ App), appeal denied, 683 A2d 1163 (NJ 1996). 1996. Also available online. Last accessed February 26, 2020.[PUBMED Abstract]
- Molloy v. Meier, Nos. C9-02-1821, C2-02-1837 (Minn 2004). 2004. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- Health Insurance Portability and Accountability Act of 1996, Public Law 104-191, 104th Congress. Washington, DC: 1996. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- US Department of Health and Human Services: OCR Privacy Brief: Summary of the HIPAA Privacy Rule. Washington, DC: US Department of Health and Human Services, 2002. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- Gordijn B: Genetic diagnosis, confidentiality and counseling: an ethics committee's potential deliberations about the do's and don'ts. HEC Forum 19 (4): 303-12, 2007.[PUBMED Abstract]
- Robson ME, Storm CD, Weitzel J, et al.: American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol 28 (5): 893-901, 2010.[PUBMED Abstract]
- Robson ME, Bradbury AR, Arun B, et al.: American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. J Clin Oncol 33 (31): 3660-7, 2015.[PUBMED Abstract]
- National Society of Genetic Counselors: National Society of Genetic Counselors Code of Ethics. Chicago, Il: National Society of Genetic Counselors, 2006. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- International Society of Nurses in Genetics: Position Statements: Privacy and Confidentiality of Genetic Information: The Role of the Nurse. Pittsburgh, Pa: International Society of Nurses in Genetics, 2010. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- US President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research: Screening and Counseling for Genetic Conditions: The Ethical, Social, and Legal Implications of Genetic Screening, Counseling, and Education Programs. Washington, DC: Government Printing Office, 1983. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- ASHG statement. Professional disclosure of familial genetic information. The American Society of Human Genetics Social Issues Subcommittee on Familial Disclosure. Am J Hum Genet 62 (2): 474-83, 1998.[PUBMED Abstract]
- Lowrey KM: Legal and ethical issues in cancer genetics nursing. Semin Oncol Nurs 20 (3): 203-8, 2004.[PUBMED Abstract]
- Wauters A, Van Hoyweghen I: Global trends on fears and concerns of genetic discrimination: a systematic literature review. J Hum Genet 61 (4): 275-82, 2016.[PUBMED Abstract]
- Prince AE, Roche MI: Genetic information, non-discrimination, and privacy protections in genetic counseling practice. J Genet Couns 23 (6): 891-902, 2014.[PUBMED Abstract]
- National Conference of State Legislatures: Summary: Selected Health Legislation 110th Congress. Washington, DC: National Conference of State Legislatures, 2008. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- National Human Genome Research Institute: National Human Genome Research Institute Genome Statute and Legislation Database. Bethesda, Md: National Humokayan Genome Research Institute, 2008. Also available online. Last accessed February 27, 2020.[PUBMED Abstract]
- Leib JR, Hoodfar E, Haidle JL, et al.: The new genetic privacy law: how GINA will affect patients seeking counseling and testing for inherited cancer risk. Community Oncology 5 (6): 351-4, 2008.[PUBMED Abstract]
- Asmonga D: Getting to know GINA. An overview of the Genetic Information Nondiscrimination Act. J AHIMA 79 (7): 18, 20, 22, 2008.[PUBMED Abstract]
- National Human Genome Research Institute: "GINA": The Genetic Information Nondiscrimination Act of 2008: Information for Researchers and Health Care Professionals. Bethesda, MD: National Human Genome Research Institute, 2009. Available online. Last accessed February 27, 2020.[PUBMED Abstract]
- United States Department of Labor: Frequently Asked Questions Regarding the Genetic Information Nondiscrimination Act. Washington, DC: United States Department of Labor, 2010. Available online. Last accessed February 27, 2020.[PUBMED Abstract]
- U.S. Equal Employment Opportunity Commission: The Genetic Information Nondiscrimination Act of 2008. Washington, DC: U.S. Equal Employment Opportunity Commission, 2008. Available online. Last accessed February 27, 2020.[PUBMED Abstract]
- Parkman AA, Foland J, Anderson B, et al.: Public awareness of genetic nondiscrimination laws in four states and perceived importance of life insurance protections. J Genet Couns 24 (3): 512-21, 2015.[PUBMED Abstract]
- Green RC, Lautenbach D, McGuire AL: GINA, genetic discrimination, and genomic medicine. N Engl J Med 372 (5): 397-9, 2015.[PUBMED Abstract]
- Allain DC, Friedman S, Senter L: Consumer awareness and attitudes about insurance discrimination post enactment of the Genetic Information Nondiscrimination Act. Fam Cancer 11 (4): 637-44, 2012.[PUBMED Abstract]
- Hudson KL, Holohan MK, Collins FS: Keeping pace with the times--the Genetic Information Nondiscrimination Act of 2008. N Engl J Med 358 (25): 2661-3, 2008.[PUBMED Abstract]
- Baruch S, Hudson K: Civilian and military genetics: nondiscrimination policy in a post-GINA world. Am J Hum Genet 83 (4): 435-44, 2008.[PUBMED Abstract]
- Changes to This Summary (05/08/2020)
-
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Cancer Genetics Service Delivery
Added this new section.
This summary is written and maintained by the PDQ Cancer Genetics Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® - NCI's Comprehensive Cancer Database pages.
- About This PDQ Summary
-
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about cancer genetics risk assessment and counseling. It is intended as a resource to inform and assist clinicians who care for cancer patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Cancer Genetics Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website's Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Cancer Genetics Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Cancer Genetics Editorial Board. PDQ Cancer Genetics Risk Assessment and Counseling. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/about-cancer/causes-prevention/genetics/risk-assessment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389258]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
The information in these summaries should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.